

When we think about what makes cities possible, agriculture usually gets top billing. Without a steady food surplus, people could not have stopped foraging long enough to become artisans, priests, merchants, or kings. But once people clustered into towns and cities, another, less glamorous need quickly emerged: what to do with all the waste. While no one likes to think about it, without effective methods for sewage disposal cities would quickly become uninhabitable.
When you consider the foundations of modern civilization, sewers probably don’t make your top ten list. But these underground networks deserve way more credit than they get. It is no exaggeration to say that sewage systems—whether open drains in the street or vast subterranean tunnels—were one of the most important technologies that made large cities livable. The story of sewers is really the story of how humans figured out how to live together in large numbers without, well, dying from our own waste.
The Ancient World Gets Creative
The earliest cities faced a pretty basic problem: what do you do with human and animal waste when you’ve got thousands of people living close together? The ancient Indus Valley civilization (around 2600-1900 BCE) came up with one of the first solutions. Archaeological evidence from Harappa and Mohenjo-daro shows they built covered drains and even had individual house connections—pretty impressive for 4,000 years ago.
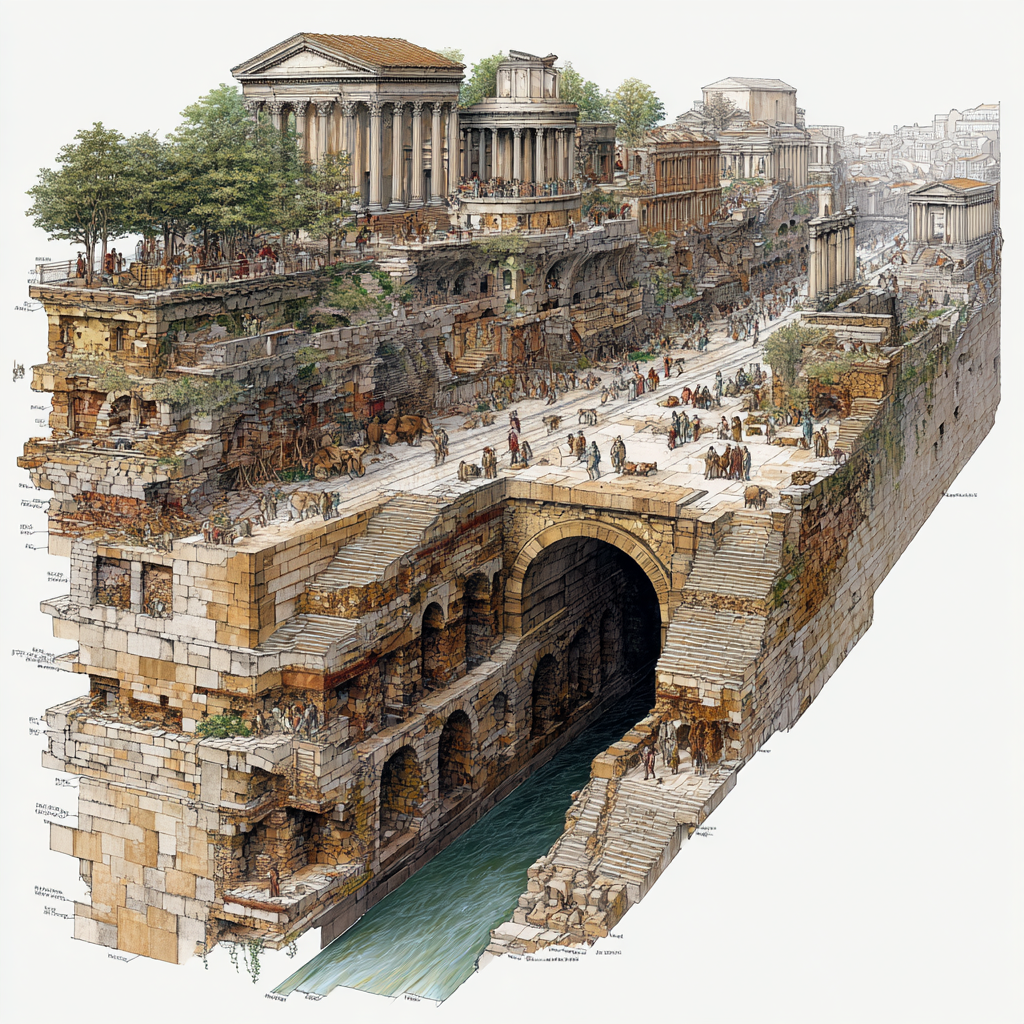
The Romans, being Romans, took this concept and ran with it. The Cloaca Maxima, built around 600 BCE, started as an open drainage canal but eventually became Rome’s main sewer system. What made Roman sewers special wasn’t just their size, but how they integrated with aqueducts to create a flow-through system that actually worked.
Speculation alert: While we know the Romans understood the practical benefits of sewers, they probably didn’t fully grasp the disease prevention aspect in the way we do today.
The Medieval Mess
After Rome fell, European cities pretty much forgot how to manage waste properly. Medieval cities relied on a charming system where people just dumped waste into the streets, hoping rain would wash it away. Some cities built latrines that emptied into rivers, but most urban waste management was… let’s call it “informal.”
This wasn’t just gross—it was deadly. Cities regularly faced outbreaks of cholera, dysentery, and typhoid, though people didn’t yet understand the connection between contaminated water and disease.
London’s Wake-Up Call
The turning point came in 19th-century London. By the 1850s, the Thames had become essentially an open sewer, and the city’s water supply was contaminated. The “Great Stink” of 1858 made the problem impossible to ignore. The smell from the Thames was so bad that Parliament couldn’t meet. When something smells worse than politics you know that’s bad.
Enter Joseph Bazalgette, chief engineer of London’s Metropolitan Board of Works. His solution was ambitious: build a comprehensive sewer network that would intercept waste before it reached the Thames and carry it downstream to treatment facilities. The system, completed in the 1870s, used gravity and the natural slope of the land to move waste through a network of tunnels—some large enough to drive a carriage through.
Who wouldn’t love the idea that a man named Thomas Crapper invented the flush toilet. But that’s not quite true. Variations of the flush toilet have been around for over 2000 years. In 1775, a man named Alexander Cummings invented the S-trap—a curved pipe that prevented sewer gases from backing up into the home—making toilets finally tolerable for indoor use. While Mr. Crapper did not invent the toilet, he did make it functional enough to be routinely installed in homes by creating a workable ballcock mechanism to allow reliable flushing. He also marketed a toilet of his own design, leading to the now familiar nickname of “the crapper.”
Reversing A River
Chicago’s development of a sewer system was a landmark feat of engineering and urban planning in the 19th century. Faced with flat, swampy terrain and rapid population growth, the city recruited engineer Ellis S. Chesbrough in 1855 to design the first comprehensive underground sewer system in the United States. Because the landscape offered little natural drainage, the entire city center had to be physically raised by several feet—an ambitious task that involved elevating streets and even entire buildings above their original grade to allow for gravity-based drainage into the Chicago River.
Apparently, no one realized this would pollute Lake Michigan, the city’s main drinking water source, a classic example of unintended consequences. This led to further innovation, including the construction of a tunnel extending two miles under the lake to bring in cleaner water (completed in 1866) and, ultimately, the monumental reversal of the Chicago River’s flow in 1900. This project diverted wastewater away from the lake and toward the Mississippi basin, following the time-tested political solution of sending your problems downstream.
The Science Behind the Solution
What made modern sewer systems revolutionary wasn’t just engineering—it was the growing understanding of how disease spreads. Dr. John Snow’s work during London’s 1854 cholera outbreak proved that contaminated water, not “bad air,” was spreading the disease. This discovery gave city planners the scientific backing they needed to invest heavily in sewer infrastructure.
Modern sewer systems work on relatively simple principles: gravity moves waste through sloped pipes to treatment facilities, where biological and chemical processes break down harmful materials before releasing treated water back into the environment. The key innovation was creating separate systems for stormwater and sewage, preventing overflow during heavy rains.
Cities Transform
The impact was immediate and dramatic. Cities with comprehensive sewer systems saw massive drops in waterborne diseases. Life expectancy increased, child mortality plummeted, and for the first time in human history, really large cities became livable spaces rather than death traps.
Sewers enabled urban growth on an unprecedented scale. Without sewers, cities like New York, Chicago, and London couldn’t support populations in the millions. The investment in underground infrastructure became the foundation for everything else—commerce, industry, culture—that makes cities economic powerhouses.
Modern Challenges
Today’s sewer systems face new challenges. Climate change brings more intense storms that can overwhelm older systems. Growing populations strain infrastructure that was built decades ago. Many cities are dealing with the expensive reality that sewer systems, built to last 50-100 years have outlived their life expectancy and need major upgrades or replacement.
Prediction: Cities will likely need to invest heavily in “smart” sewer systems over the next few decades—networks that use sensors and data to manage flow more efficiently and prevent overflows.
The Bottom Line
Sewers represent one of humanity’s most important but least appreciated innovations. They made modern urban life possible by solving the fundamental problem of waste management on a large scale. Without this underground network, our cities and the economic and cultural benefits they provide simply couldn’t exist.
The next time you turn on a tap or use indoor plumbing, remember you’re benefiting from centuries of engineering innovation that literally built the foundation of modern civilization, one pipe at a time.
Sometimes when I’m researching articles, I find myself going down a rabbit hole. This time I went down the drain.






The Correlation Mirage: How Good Intentions Go Wrong in Health Debates
By John Turley
On December 8, 2025
In Commentary, Medicine
Understanding the Basics
Here’s the fundamental problem: just because two things happen together doesn’t mean one caused the other. When we say two variables are “correlated,” we’re simply observing that they move in tandem—when one goes up, the other tends to go up (or down). Causation, on the other hand, means that a change in one variable directly causes a change in the other. Think of correlation as a suspicious coincidence, while causation is a proven relationship with a clear mechanism.
The tricky part is that our brains are pattern-seeking machines. We evolved to spot connections quickly because that helped our ancestors survive. If you ate those red berries and got sick, better to assume the berries caused it rather than to wait around for a controlled study. But this mental shortcut can seriously mislead us in the modern world, especially when it comes to complex health issues.
Classic Examples That Illustrate the Problem
Let me give you some examples that show how ridiculous this confusion can get when we’re not careful. There’s a famous correlation between ice cream sales and drowning—both increase during summer months, but ice cream isn’t causing drowning. The real driver is warmer weather, which leads people to both buy more ice cream and to spend more time at beaches or swimming pools where drowning might happen. This is what researchers call a “confounding variable”—a third factor that influences both things you’re measuring.
Here’s another head-scratcher: there’s a correlation between the number of master’s degrees awarded and box office revenue. Does getting more education somehow boost movie sales? Of course not. This is what we call a spurious correlation—a completely coincidental relationship that exists in the data but has no meaningful connection in reality.
Here’s good news for us coffee drinkers. For years, studies suggested a correlation between heavy coffee drinking and heart disease. Later research found the real issue: heavy coffee drinkers were also more likely to smoke. Once smoking was controlled for, coffee itself did not increase heart risk.
Perhaps the most amusing example is the correlation between stork populations and birth rates in Germany and Denmark spanning decades. As the stork population fluctuated, so did the number of newborns. Now, you could construct a “Theory of the Stork” claiming that storks deliver babies, but the real explanation probably involves other variables like weather patterns, urbanization, or environmental developments that affected both populations.
The medical field offers more serious examples. You observe a strong correlation between exercise and skin cancer cases—people who exercise more seem to get skin cancer at higher rates. Without digging deeper, you might panic and conclude that exercise somehow causes cancer. But the actual explanation is far more mundane: people who exercise more tend to spend more time outdoors in the sun, which increases their UV exposure. The confounding variable here is sun exposure, not the exercise itself.
The Vaccine-Autism Controversy: A Cautionary Tale
Now let’s talk about one of the most damaging correlation-causation confusions in recent medical history: the claim that vaccines cause autism. Many childhood vaccines are administered at the same ages when numerous developmental conditions first become noticeable—including autism, seizure disorders, and certain metabolic or genetic issues. This is a textbook case of how mistaking correlation for causation can have real-world consequences.
The whole mess started in 1998 when Andrew Wakefield, a gastroenterologist at London’s Royal Free Hospital, published a paper in The Lancet describing 12 children, eight of whom were reported as having developed autism after receiving the MMR vaccine. Here’s the thing: this wasn’t even a proper study that could establish causation. It was described as a consecutive case series with no control group or control period—it was simply a description that couldn’t tell you whether one thing causes another.
But why did this idea catch fire so dramatically? The timing created a perfect storm for correlation-causation confusion. Autism becomes apparent early in childhood, around the same time children receive many vaccines and there will be a temporal relationship by chance alone. Parents naturally searched for explanations, noticed the temporal proximity, and drew what seemed like an obvious conclusion.
The scientific community took these concerns seriously and conducted extensive research. Despite overwhelming data demonstrating that there is no link between vaccines and autism, many parents remain hesitant to immunize their children because of the alleged association. Study after study found no connection. A study of over 500,000 children in Denmark, published in The New England Journal of Medicine in 2002 found no relationship between autism and MMR as did a subsequent Danish study published in 2019. In April 2015, JAMA published a large study analyzing health records of over 95,000 children, including about 2,000 who were at risk for autism because they had a sibling already diagnosed. It confirmed that the MMR vaccine did not increase the risk for autism spectrum disorder.
The original Wakefield study eventually collapsed under scrutiny. The Lancet retracted the article, and Wakefield was found guilty of deliberate fraud—he picked and chose data that suited his case and falsified facts. Wakefield lost his license to practice medicine after being sanctioned by scientific bodies. But by then, the damage was done.
Here’s the correlation-causation issue in stark terms: the prevalence of autism has increased over time, which researchers and healthcare professionals explain is likely due to multiple factors, including people becoming more aware of autism, improved screening, and updated and expanded diagnostic criteria to include other conditions on the autism spectrum. Meanwhile, immunizations have increased and have dramatically reduced the incidence of vaccine-preventable diseases. These two trends—increasing autism diagnoses and increasing vaccination rates—happened to occur during the same historical period, creating an illusory correlation.
The real causes of autism are complex. There is no single root cause; a combination of influences is likely involved, including certain genetic syndromes, genetic changes affecting cell function, and environmental influences such as premature birth, older parents, and illness during pregnancy. Vaccines simply aren’t part of that picture.
Other Health-Related Confusion
The vaccine-autism controversy isn’t the only place where correlation-causation confusion causes problems in health contexts. Let me give you a few more examples that show how pervasive this issue is and how difficult it can be to distinguish between correlation and causation.
Consider the relationship between diet and health outcomes. The amount of sodium a person gets in their diet is closely correlated to the total calories they eat—in other words, the more a person eats, the more sodium they’re likely to take in, and eating a lot of calories often leads to obesity. Both obesity and high-sodium diets are believed to contribute to high blood pressure. So, what’s the primary driver? Is it sodium, excess calories, or obesity? These are exactly the kinds of questions researchers must carefully untangle.
Here’s another tricky one: research has shown a correlation between antibiotic use in children and increased risk of obesity, with greater antibiotic use associated with higher obesity risk, particularly for children with four or more exposures. But this correlation alone doesn’t tell us whether antibiotics cause obesity. There could be multiple explanations: perhaps children who need frequent antibiotics have other health issues that predispose them to weight gain, or perhaps the infections themselves (not the antibiotics) are the real issue, or maybe it’s actually a disruption of gut bacteria that matters. Without understanding the exact physiological mechanism, we can’t design effective interventions.
Similarly, increased BMI seems to be associated with an increased risk of several cancers in adults. But it would be erroneous to conclude that simply being overweight directly causes cancer. Socioeconomic factors, environmental toxins, access to healthcare, lifestyle differences, physical activity levels, and diet all intertwine in complex ways. Some people may face multiple risk factors simultaneously, making it difficult to isolate which factors are most significant.
When cell phones first became widely used, there was an increasing concern that radiation from the cell phones was causing brain cancer. Brain cancer rates have remained stable for decades despite exponential increases in cell-phone use—strong evidence against a causal relationship.
Beyond Statistics
The stakes here go way beyond academic accuracy. When people confuse correlation with causation in health contexts, they make decisions that can harm themselves and others. The 2017 measles epidemic in Minnesota’s Somali community was in no small measure fomented by Wakefield—he didn’t fade away quietly. He and other anti-vaxers repeatedly proselytized to the community, leading to an approximately 45% reduction in vaccination. At the same time there was an increase in autism diagnoses. Think about that: vaccination rates dropped, yet autism diagnoses continued to rise—the exact opposite of what you’d expect if vaccines caused autism. A word of caution: this is an observation, not a carefully controlled study.
The problem extends to how we evaluate new treatments and risk factors. In clinical medicine, there are treatment protocols in use that are not supported by randomized controlled trials. There are risk factors that have been associated with various diseases where it’s difficult to know for certain if they are actually contributing causes. This uncertainty creates space for misunderstanding.
How Scientists Establish Causation
So, how do researchers move from observing a correlation to proving causation? They look for several key elements. These include: a stronger association between variables (which is more suggestive of cause and effect than a weaker one), proper temporality (the alleged effect must follow the suspected cause), a dose-response relationship (where increasing exposure leads to proportionally greater effects), and a biologically plausible mechanism of action.
The gold standard is the randomized controlled trial, where researchers can carefully control for confounding variables by randomly assigning people to treatment and control groups. For ethical reasons, there are limits to controlled studies—it wouldn’t be appropriate to use two comparable groups and have one undergo a harmful activity while the other does not. That’s why we often rely on observational studies combined with careful statistical methods to rule out alternative explanations.
The Bottom Line
Understanding the difference between correlation and causation isn’t just an academic exercise—it’s a critical thinking skill that helps you navigate health claims, news stories, and medical decisions. The vaccine-autism controversy shows how dangerous it can be when we mistake coincidental timing for causal relationships, especially when those misunderstandings spread through communities and lead to preventable disease outbreaks.
The key takeaway? When you see two things happening together, your brain will want to assume one caused the other. Resist that urge. Ask yourself: could there be a third factor driving both? Could the timing just be coincidental? Is there a clear, testable mechanism that would explain how one causes the other? These questions can help you separate meaningful connections from statistical coincidences—and potentially save you from making poor health decisions based on faulty reasoning.