When Fat in the Blood Runs in the Family
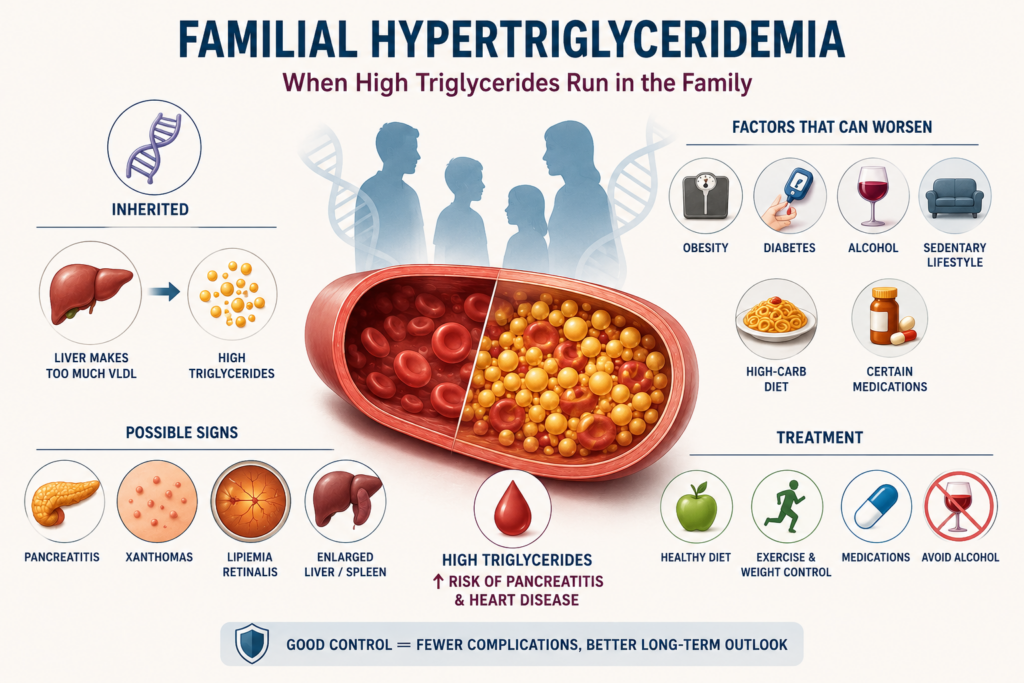
Most people know they should keep an eye on their cholesterol. But triglycerides — another type of fat circulating in the blood — often fly under the radar. For some families, though, high triglycerides aren’t just a lifestyle problem. They’re baked into the DNA. Familial hypertriglyceridemia (FHTG) is a hereditary condition in which the liver chronically overproduces fat-carrying particles, sending triglyceride levels well above what diet alone can fully explain. It’s more common than most people realize and is frequently under diagnosed. If left unaddressed it can trigger serious complications including pancreatitis and heart disease.
One of my earliest disappointments as a young physician was a patient with familial hypertriglyceridemia. He was in his late 20s and his triglycerides were running in the critical level. We tried multiple interventions and he was referred to multiple specialists. Unfortunately, he wasn’t able to make the lifestyle changes he needed to make and progressively got worse and worse before passing away in his mid-30s. Fortunately, we have better treatments now, but this still is potentially a dangerous disease.
This article walks through FHTG, what it is, what causes it, how it presents, how it’s diagnosed, and what modern medicine can actually do about it.
What Is Familial Hypertriglyceridemia?
Triglycerides are the most common form of fat in the body. After you eat, calories that your body doesn’t immediately need are converted into triglycerides and stored in fat cells. Between meals, hormones release these fats for energy. When this system gets stuck in the “on” position — or when the body doesn’t clear triglycerides efficiently — blood levels climb.
FHTG, technically classified as Type IV familial dyslipidemia, is a genetic disorder in which the liver overproduces very low-density lipoprotein (VLDL) particles — essentially the trucks that carry triglycerides through the bloodstream. The result is persistently elevated triglyceride levels, typically in the moderate-to-severe range, sometimes severe enough to become medically dangerous.
Normal fasting triglycerides are generally below 150 mg/dL. Borderline high falls between 150 and 199. In FHTG, levels often run 200–500 mg/dL or higher, and some patients can exceed 1,000 mg/dL, a threshold at which the risk of acute pancreatitis rises sharply.
Etiology: The Genetic Story Is More Complicated Than Expected
For decades, FHTG was described in textbooks as a straightforward autosomal dominant disorder — meaning one copy of a faulty gene was enough to cause the condition, and each child of an affected parent had a 50% chance of inheriting it. That picture has been substantially revised by modern genetics.
It turns out that FHTG is primarily polygenic — driven not by a single dramatic mutation but by the cumulative effect of many small genetic variants. Studies have now identified more than 300 independent genetic locations associated with plasma triglyceride levels. No single gene tells the whole story. Instead, a person inherits a kind of genetic “load” that creates susceptibility — and whether that susceptibility becomes clinically apparent often depends on environmental triggers.
The genes involved all play a role in how the body metabolizes fat-carrying particles. Heterozygous (single-copy) variants in these genes are common in most FHTG patients. The much rarer and more severe familial chylomicronemia syndrome (FCS) both copies are defective producing extreme triglyceride elevations and a very different clinical picture.
Environmental factors that worsen FHTG include obesity, poorly controlled diabetes, alcohol use, a diet heavy in refined carbohydrates and sugars, estrogen-containing medications, and certain drugs such as corticosteroids and beta-blockers. In many patients, the genetic predisposition only becomes clinically obvious when one or more of these environmental triggers is present — which explains why the condition often goes undetected until adulthood.
Symptoms: The Quiet Condition
One of FHTG’s most deceptive features is that it is often silent. Many people carry the condition for years without a single symptom, discovering it only through routine blood work or a family history investigation. This is why widespread lipid screening is so important — FHTG doesn’t announce itself with chest pain or obvious physical signs, at least not initially.
When symptoms first appear, they are often subtle and tend to reflect either the degree of triglyceride elevation or the presence of associated conditions. In cases of moderate elevation, patients might experience vague fatigue, weight gain, or features of metabolic syndrome — high blood pressure, elevated blood sugar, increased waist circumference.
At higher triglyceride levels, more distinctive signs can emerge. Xanthomas, yellowish, waxy deposits of fat under the skin, may appear, particularly around the eyelids (xanthelasmas) or over the elbows, knees, or tendons. The liver may enlarge (hepatomegaly), reflecting fat accumulation. An eye exam may show lipemia retinalis — a milky or salmon-pink discoloration of the retinal blood vessels — visible with an ophthalmoscope when triglycerides are extremely high.
The most dangerous symptom is severe abdominal pain signaling acute pancreatitis. When triglycerides exceed 1,000 mg/dL, the pancreas can become inflamed as it is overwhelmed by fat-rich particles. This is a medical emergency. Nausea, vomiting, and upper abdominal pain radiating to the back are warning signs that warrant immediate evaluation.
There is also an increased risk of early cardiovascular disease in FHTG patients, particularly when metabolic syndrome is present, though the relationship between triglycerides alone and heart disease risk is more nuanced than it is with LDL cholesterol.
Diagnosis: Getting the Full Picture
Diagnosis begins with a standard fasting lipid panel — a blood test that measures total cholesterol, LDL, HDL, and triglycerides. In FHTG, the hallmark findings are elevated triglycerides and VLDL, often accompanied by low HDL (the so-called “good” cholesterol). LDL levels may be normal or even low, which can sometimes falsely reassure both patients and physicians.
Because many things can raise triglycerides — including a meal eaten before the blood draw, excess alcohol, diabetes, hypothyroidism, kidney disease, and certain medications — the first step is ruling out secondary causes. A thorough personal and family history is essential. A clinician who asks about triglycerides in parents or siblings or even children is doing exactly what the guidelines recommend.
The “familial” part of the diagnosis is confirmed when multiple first-degree relatives are found to have elevated triglycerides, when the elevation persists despite controlling for secondary causes, and when the pattern fits what we’d expect from a heritable condition appearing across generations.
Genetic testing can identify specific variants in the related genes, but it is not required for a clinical diagnosis and is not routinely performed. Genetic testing may be ordered when the clinical picture is severe or ambiguous, or when distinguishing FHTG from the rarer familial chylomicronemia syndrome which has treatment implications such as the emerging targeted therapies.
Current guidelines also recommend evaluating for cardiovascular risk in patients with mild-to-moderate FHTG, and for pancreatitis risk in those with severe elevations.
Treatment: A Layered Approach
Lifestyle First
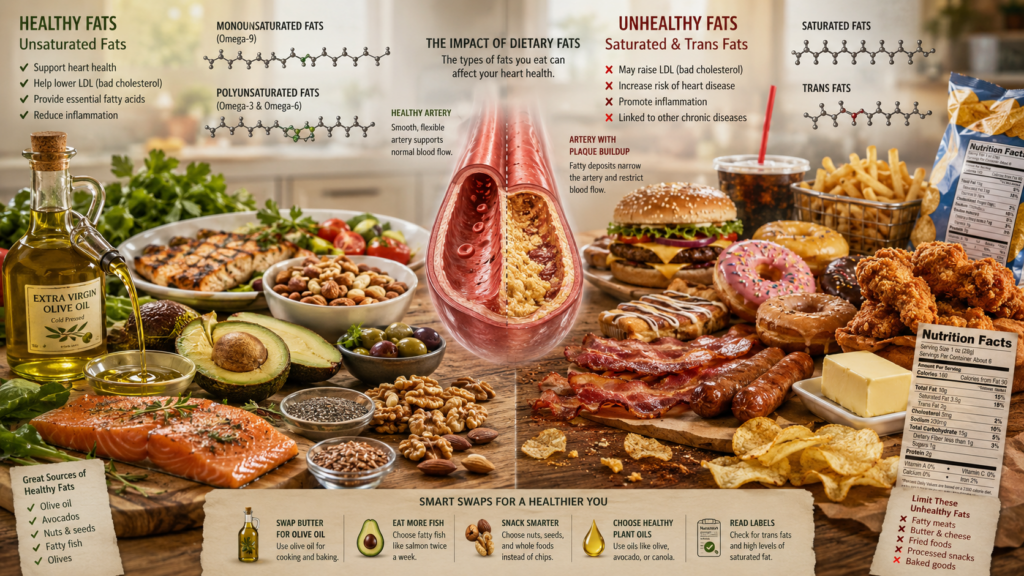
The cornerstone of FHTG management — at least for mild-to-moderate disease — is lifestyle modification, and it can be remarkably effective. Cutting refined carbohydrates and added sugars is particularly powerful. Saturated fat primarily raises LDL cholesterol, but it is carbohydrates that drive hepatic triglyceride production. Alcohol is another major player. Even moderate consumption can substantially raise triglycerides in susceptible individuals, and abstinence often produces dramatic improvements.
Weight loss, regular aerobic exercise, and tight blood sugar control in patients with diabetes or prediabetes round out the lifestyle toolkit. Estrogen-containing contraceptives or hormone replacement therapy should be reconsidered in women with FHTG, as estrogen directly stimulates hepatic VLDL production and can push levels dangerously high.
Pharmacologic Options
When lifestyle changes aren’t enough, several drug classes are available. Fibrates (such as fenofibrate and gemfibrozil) are the most established triglyceride-lowering medications and can reduce levels by 30–50%. They work primarily by activating receptors that enhance triglyceride clearance.
Omega-3 fatty acids at prescription doses (2–4 grams per day) provide another option. High dose eicosapentaenoic acid (EPA), specifically the formulation icosapent ethyl (Vascepa), has demonstrated cardiovascular benefit in a major clinical trial in high-risk patients with elevated triglycerides who are already on statin therapy.
Niacin (nicotinic acid) was once widely used but has fallen out of favor after clinical trials failed to show cardiovascular benefit on top of statin therapy, despite its triglyceride-lowering ability. It is also poorly tolerated due to its side effect profile and patients frequently are noncompliant.
Statins are prescribed primarily to manage cardiovascular risk and LDL cholesterol rather than to lower triglycerides directly, though they have a modest effect on the latter.
Emerging Therapies
Perhaps the most exciting development in recent years is the arrival of RNA-based medications targeting apolipoprotein C-III (APOC3) — a protein that inhibits the clearance of triglyceride-rich particles. By silencing the gene that produces APOC3, these drugs can achieve dramatic reductions in triglyceride levels even in patients who don’t respond to conventional therapies.
Olezarsen received FDA approval in 2024 for patients with familial chylomicronemia syndrome. Its application in FHTG more broadly is an active area of clinical investigation. Similarly, drugs targeting angiopoietin-like proteins are under study, offering the prospect of precision medicine approaches to a condition that has long resisted fully effective treatment.
Prognosis: Manageable, But Not to Be Ignored
The prognosis for FHTG is generally favorable when the condition is identified and managed appropriately. Unlike some other inherited lipid disorders, FHTG is not automatically associated with dramatically elevated cardiovascular risk — particularly when LDL and HDL levels are otherwise reasonable. This distinguishes it from conditions like familial hypercholesterolemia, where premature heart disease is nearly inevitable without treatment.
That said, FHTG patients frequently carry additional cardiovascular risk factors as part of the metabolic syndrome package that must be addressed in its own right. The American Heart Association has noted that this clustering of risk factors likely elevates cardiovascular risk in FHTG patients beyond what triglycerides alone would predict.
The more immediate and measurable danger in FHTG is pancreatitis. When triglycerides are severely elevated, the risk of a potentially life-threatening inflammatory episode of the pancreas is real. Repeated bouts of pancreatitis can cause chronic damage, that impairs digestive function and increases the risk of pancreatic cancer. Preventing severe hypertriglyceridemia through consistent management — lifestyle, medication, or both — is not optional for high-risk patients.
With appropriate care, most patients with FHTG can expect to live a normal lifespan. The key predictors of outcome are compliance with dietary and lifestyle changes, appropriate use of medication when indicated, regular lipid monitoring, and attention to comorbidities like diabetes and hypertension. Family members of affected individuals also should be screened.
Bottom Line
Familial hypertriglyceridemia is one of those conditions that rewards attention and penalizes neglect. It runs quietly in families, often masked by other lifestyle factors until a crisis — a pancreatitis episode, an unexpected cardiovascular event — brings it to light. Modern genetics has revealed it to be more complex than once thought, driven by a mosaic of variants rather than a single defective gene. Treatment has evolved accordingly: from basic dietary counseling to sophisticated RNA-based drugs that target the fat metabolism pathway at the molecular level.
If you have a family history of high triglycerides, early heart disease, or pancreatitis of unclear cause, it’s worth having a conversation with your doctor about a fasting lipid panel and a careful family history review. Knowing is the first step to managing.
Medical Disclaimer
The information provided in this article is intended for general educational and informational purposes only and does not constitute medical advice. It should not be used as a substitute for professional medical advice, diagnosis, or treatment.
Always seek the guidance of a qualified healthcare provider with any questions you may have regarding a medical condition or treatment. Never disregard professional medical advice or delay seeking it because of something you have read here.
If you are experiencing a medical emergency, call 911 or your local emergency number immediately.
The author of this article is a licensed physician, but the views expressed here are solely those of the author and do not represent the official position of any hospital, health system, or medical organization with which the author may be affiliated.
Image generated by author using ChatGPT.
Sources
• MedlinePlus – Familial Hypertriglyceridemia
• NCBI StatPearls – Familial Hypertriglyceridemia (2024)
• Wikipedia – Familial Hypertriglyceridemia
• PMC – Genetics of Hypertriglyceridemia (Dron & Hegele, 2020)
• PMC – Understanding Hypertriglyceridemia: Integrating Genetic Insights (2024)
• PMC – Diagnosis and Treatment of Hypertriglyceridemia
• PMC – Severe Hypertriglyceridemia and Chylomicronemia Syndrome
• PMC – Pancreatic and Cardiometabolic Complications of Severe Hypertriglyceridemia (2024)
• Springer – The Genetic Basis of Hypertriglyceridemia
• Medscape – Hypertriglyceridemia: Background, Etiology, Pathophysiology
• PMC – Olezarsen for Familial Chylomicronemia Syndrome (2024-2025)
• Endocrine Society – Evaluation and Treatment of Hypertriglyceridemia (Clinical Practice Guideline)
• Cleveland Clinic – Hypertriglyceridemia: Causes, Risk Factors & Treatment