Growing older is often described as a gradual process, but many of the body’s changes begin earlier than most people realize. By our thirties, we slowly begin to lose muscle mass. By our fifties and sixties, our metabolism slows, bones become more fragile, digestion changes, and our bodies become less efficient at absorbing certain nutrients. None of this means declining health is inevitable. In fact, one of the most powerful tools for maintaining strength, independence, and quality of life is something we do every day: eat.
The nutritional needs of older adults are different from those of younger adults—not because the body suddenly requires exotic foods or expensive supplements, but because it becomes less forgiving of nutritional shortfalls. While calorie requirements often decline as physical activity decreases and muscle mass diminishes, the need for high-quality nutrients remains the same or even increases. Nutritionists refer to this as the challenge of nutrient density: getting more nutrition from fewer calories.
The goal of eating well in later life is not simply to prevent disease. It is to preserve muscle, maintain cognitive function, support the immune system, protect the heart and bones, and help people remain active and independent for as long as possible.
Protein: The Cornerstone of Healthy Aging
Protein is perhaps the most important of all nutrients as we age. Beginning around age 30, adults lose approximately 3 to 8 percent of their muscle mass each decade. After age 60, the rate often accelerates. This gradual decline, known as sarcopenia, contributes to weakness, slower walking speed, impaired balance, increased risk of falls, and loss of independence. During illness or hospitalization, muscle can disappear surprisingly quickly, making recovery more difficult.
The problem is compounded by what scientists call anabolic resistance. Aging muscle simply does not respond to protein as efficiently as younger muscle. Older adults must consume more protein—and distribute it more evenly throughout the day—to stimulate muscle repair and growth.
The Recommended Dietary Allowance is 0.8 grams of protein per kilogram of body weight— that’s about 80 grams for a 160-pound adult. For reference, a 4 oz serving of salmon has about 22 grams of protein. Many geriatric nutrition experts recommend 1.0 to 1.2 grams per kilogram daily for healthy adults over age 65. Those recovering from surgery, injury, or serious illness may require1.2 to 1.5 grams per kilogram, but only under medical supervision.
Equally important is timing. Many Americans consume very little protein at breakfast, a modest amount at lunch, and most of it at dinner. Research suggests muscle responds better when approximately 25 to 30 grams of protein are consumed at each meal.
Excellent sources include fish, poultry, lean meat, eggs, Greek yogurt, cottage cheese, beans, lentils, tofu, soy products, nuts, and seeds. Dairy proteins such as whey are especially rich in leucine, an amino acid that plays a central role in stimulating muscle protein synthesis.
Nutrition alone, however, is only part of the equation. Resistance training—even with light weights or resistance bands—works hand in hand with adequate protein to preserve muscle throughout later life.
Carbohydrates: Choosing Quality Over Quantity
Carbohydrates have acquired an undeserved reputation in many popular diets. In reality, they remain the body’s preferred source of energy and are especially important for the brain, which relies heavily on glucose to function.
The key is not eliminating carbohydrates but selecting healthier ones.
As we age, our bodies often become less sensitive to insulin, making blood sugar regulation more challenging. Highly refined carbohydrates—white bread, pastries, sugary beverages, and many processed snack foods—cause rapid spikes in blood glucose followed by equally rapid declines. Over time, these fluctuations may contribute to weight gain, insulin resistance, and type 2 diabetes.
Complex carbohydrates digest more slowly, providing a steadier release of energy while supplying vitamins, minerals, and fiber. Whole grains such as oatmeal, barley, brown rice, and whole-wheat bread are excellent choices. Fruits, vegetables, beans, and lentils provide carbohydrates along with antioxidants and phytochemicals that support overall health.
Contrary to popular belief, potatoes are not inherently unhealthy. Preparation matters. A baked potato with its skin offers potassium, vitamin C, and fiber, whereas deep-fried potatoes or heavily buttered mashed potatoes provide considerably more calories and saturated fat.
Many older adults find that emphasizing minimally processed carbohydrates improves energy levels and helps maintain stable blood sugar throughout the day.
Fiber: The Unsung Hero
Fiber is one of the most overlooked nutrients in the American diet, yet it becomes increasingly important with age.
Digestive motility naturally slows as we grow older. Physical inactivity, inadequate fluid intake, and medications—including opioid pain relievers, some antidepressants, calcium supplements, and certain blood pressure medications—can further contribute to constipation.
Fiber helps keep the digestive system functioning normally by increasing stool bulk and promoting regular bowel movements. But its benefits extend well beyond the gastrointestinal tract.
A high-fiber diet lowers LDL (“bad”) cholesterol, slows glucose absorption, improves blood sugar control, supports healthy gut bacteria, and increases feelings of fullness, helping many people maintain a healthy weight.
Current recommendations suggest approximately 30 grams of fiber daily for older men and about 21 grams for older women, although most Americans consume substantially less.
Good sources include fresh fruits, vegetables, legumes, oats, bran cereals, nuts, seeds, and whole grains.
Fiber should always be increased gradually while maintaining adequate fluid intake. Without sufficient water, increasing fiber can actually worsen constipation.
Healthy Fats Continue to Matter
Fat remains an essential nutrient throughout life.
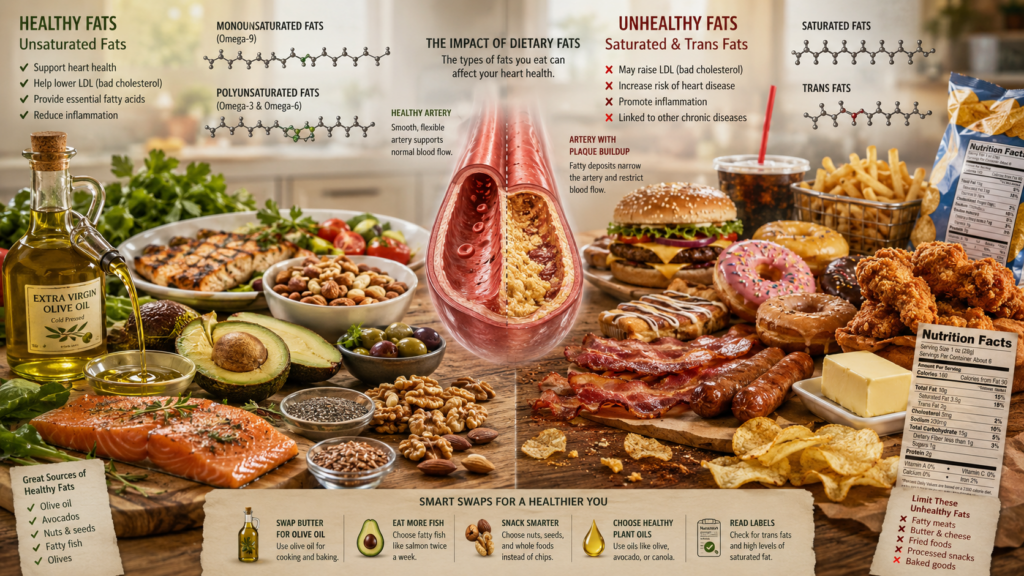
Healthy fats provide energy, help build cell membranes, assist in hormone production, reduce inflammation, and allow absorption of the fat-soluble vitamins A, D, E, and K.
Perhaps most importantly, healthy fats support cardiovascular health, an increasingly important consideration with advancing age.
Monounsaturated fats found in olive oil, avocados, almonds, pecans, pistachios, and peanuts remain among the healthiest dietary choices.
Particularly valuable are the marine omega-3 fatty acids EPA and DHA found in salmon, trout, sardines, herring, and mackerel. Numerous studies have shown that these fats lower triglyceride levels and are associated with improved cardiovascular health. Some research also suggests they may help preserve cognitive function, although evidence remains mixed.
Plant sources such as flaxseed, chia seeds, walnuts, and canola oil provide alpha-linolenic acid (ALA), another beneficial omega-3 fatty acid.
By contrast, trans fats should be avoided whenever possible, while saturated fats from fatty meats, butter, and highly processed foods are best consumed in moderation.
Hydration: The Forgotten Nutrient
Water is not technically a nutrient, yet it may be one of the most important components of healthy aging.
Older adults are especially vulnerable to dehydration for several reasons. The sensation of thirst becomes less reliable with age, kidney function changes, and many medications—including diuretics—promote fluid loss. Some older individuals intentionally drink less because of concerns about urinary urgency or nighttime trips to the bathroom.
Even mild dehydration can produce fatigue, headaches, dizziness, constipation, confusion, kidney stones, urinary tract infections, and an increased risk of falls.
Unlike younger adults, older people should not rely solely on thirst as a signal for their fluid needs.
Most healthy older adults benefit from drinking fluids consistently throughout the day. Water is the best choice, but milk, tea, coffee, soups, and water-rich foods such as melons, oranges, cucumbers, tomatoes, and berries all contribute to hydration.
The color of the urine offers a practical guide. Pale yellow generally indicates adequate hydration, whereas dark yellow urine often suggests that additional fluids are needed, although certain medications and vitamins can alter urine color.
Calcium, Vitamin D, and Bone Health
Bone is living tissue that is constantly remodeled throughout life. With age, bone breakdown gradually exceeds bone formation, increasing the risk of osteoporosis and fractures.
Adequate calcium remains important, but vitamin D is equally critical because it enables calcium absorption from the intestine. Unfortunately, aging skin produces less vitamin D in response to sunlight, and many older adults spend less time outdoors.
Dairy products, fortified plant milks, canned salmon with bones, and leafy green vegetables contribute calcium, while fatty fish and fortified foods provide modest amounts of vitamin D.
Because deficiency is common, many physicians recommend vitamin D supplementation based on blood test results.
Vitamin B12: A Common but Often Silent Deficiency
Vitamin B12 deserves special attention because deficiency becomes increasingly common after age 60.
Normal absorption requires adequate stomach acid to separate vitamin B12 from proteins in food. Aging, along with medications such as proton pump inhibitors and metformin, often reduces stomach acidity.
Symptoms may develop gradually and include fatigue, numbness or tingling in the hands and feet, difficulty walking, poor balance, memory problems, depression, and anemia.
Fortunately, crystalline vitamin B12 found in supplements and fortified foods bypasses many of these absorption problems and is highly effective in preventing or correcting deficiency.
Do Supplements Become More Important?
For many older adults, the answer is yes—but only selectively.
The ideal source of nutrition remains a balanced diet rich in vegetables, fruits, whole grains, legumes, lean proteins, dairy or fortified alternatives, nuts, seeds, and healthy oils. Foods contain thousands of biologically active compounds that supplements cannot fully replicate.
Nevertheless, certain supplements become increasingly useful as people age.
Vitamin D is among the most commonly recommended because deficiency is widespread and can adversely affect bone and muscle health. Vitamin B12 supplementation is appropriate for many older adults, particularly those taking metformin or acid-suppressing medications or those with laboratory evidence of deficiency.
Calcium supplements may be useful when dietary intake is inadequate, although obtaining calcium from food is generally preferred because large supplemental doses have been associated with possible cardiovascular concerns.
Protein powders and ready-to-drink nutritional shakes can help individuals with poor appetite, difficulty chewing, chronic illness, or increased protein requirements. Whey protein is especially effective because of its high leucine content.
Omega-3 supplements may benefit individuals who rarely consume fish, although eating fish remains the preferred strategy.
One supplement attracting increasing attention is creatine monohydrate. Long used by athletes, creatine has substantial evidence supporting its ability to improve muscle strength and enhance the benefits of resistance exercise in older adults. When taken in appropriate doses by healthy individuals, it appears remarkably safe, though people with significant kidney disease should consult their physician before using it.
In contrast, the evidence for many heavily marketed anti-aging supplements—including collagen powders, testosterone boosters, proprietary muscle blends, and high-dose antioxidant formulas—is considerably weaker. Some may offer modest benefits in selected circumstances, but many lack rigorous scientific support.
See my earlier post for more information: Supplement Smarts: What Seniors Should Know Before Reaching for That Bottle
Eating for Health, Not Simply Longevity
Nutrition is not about adding years to life alone. It is about adding life to those years.
A healthy diet cannot stop aging, but it can influence how well we age. Adequate protein helps preserve muscle and independence. Healthy carbohydrates provide steady energy. Fiber supports digestive and cardiovascular health. Unsaturated fats protect the heart and nourish the brain. Proper hydration reduces illness and maintains physical and mental function. Carefully selected supplements can fill nutritional gaps when food alone is insufficient.
Perhaps the most encouraging news is that it is never too late to benefit. Studies consistently show that older adults who improve their diet, remain physically active, and maintain adequate protein intake can increase muscle strength, improve balance, reduce the risk of chronic disease, and enhance quality of life—even well into their seventies, eighties, and beyond.
The old saying that “you are what you eat” may oversimplify nutrition, but it captures an enduring truth. As the years accumulate, every meal becomes another opportunity to nourish not just the body, but the ability to continue living fully, independently, and well.
Medical Disclaimer
The information provided in this article is intended for general educational and informational purposes only and does not constitute medical advice. It should not be used as a substitute for professional medical advice, diagnosis, or treatment.
Always seek the guidance of a qualified healthcare provider with any questions you may have regarding a medical condition or treatment. Never disregard professional medical advice or delay seeking it because of something you have read here.
If you are experiencing a medical emergency, call 911 or your local emergency number immediately.
The author of this article is a licensed physician, but the views expressed here are solely those of the author and do not represent the official position of any hospital, health system, or medical organization with which the author may be affiliated.
Image generated by author using ChatGPT.
References
Bauer J, Biolo G, Cederholm T, et al. Evidence-Based Recommendations for Optimal Dietary Protein Intake in Older People. Journal of the American Medical Directors Association. 2013.
Deutz NEP, Bauer JM, Barazzoni R, et al. Protein intake and exercise for optimal muscle function with aging. Clinical Nutrition. 2014.
Volpi E, Campbell WW, Dwyer JT, et al. Is the Optimal Level of Protein Intake for Older Adults Greater Than the Recommended Dietary Allowance? The Journals of Gerontology: Series A. 2013.
U.S. Department of Agriculture & U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2025–2030. https://www.dietaryguidelines.gov
National Institute on Aging. Healthy Eating As You Get Older. https://www.nia.nih.gov/health/healthy-eating
National Institutes of Health Office of Dietary Supplements. https://ods.od.nih.gov
European Society for Clinical Nutrition and Metabolism (ESPEN). Guideline on Clinical Nutrition and Hydration in Geriatrics. https://www.espen.org