
Structure, Function, Testing, and Clinical Implications
If you’ve ever had blood drawn during a bout of illness or a workup for heart disease risk, there’s a decent chance your doctor ordered a C-reactive protein test, usually shortened to CRP. It’s one of the most widely ordered lab tests in the world. CRP is one of the body’s most sensitive early-warning systems for inflammation. Understanding where it comes from, what it does, and how doctors use it reveals a lot about how the immune system operates and why chronic low-grade inflammation has become such a central concern in modern medicine. Warning: doctor talk will follow.
A Protein With a Peculiar Origin Story
CRP was discovered almost by accident in 1930 by William Tillett and Thomas Francis, working in Oswald Avery’s laboratory at Rockefeller University. They were studying patients with acute pneumococcal pneumonia caused by the bacteria Streptococcus pneumoniae and noticed that blood from acutely ill patients caused a specific bacterial substance to clump together. That substance was the “C polysaccharide” in the bacterial cell wall, which gave the protein its name.
For decades CRP was used as a crude yes-or-no indicator of serious infection. It wasn’t until the late 20th century that more sensitive lab techniques revealed its value for detecting the subtle, chronic inflammation now linked to cardiovascular disease and opening a major new chapter in preventive medicine. I had been in practice for several years before I even became aware of CRP.
Shape Matters: The Five-Sided Structure of CRP
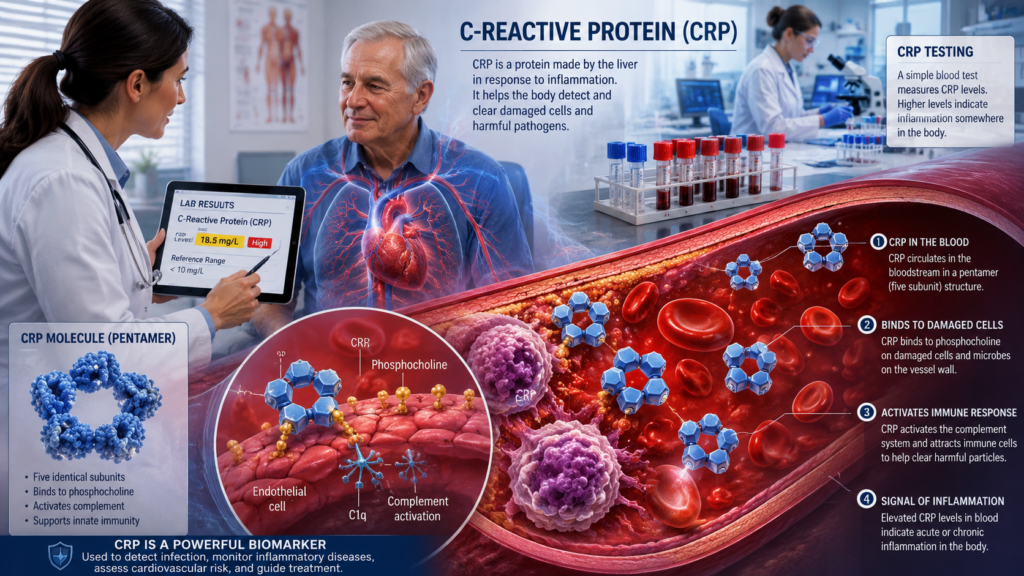
CRP belongs to a protein family called the pentraxins, named from the Greek word for “five” because of the protein’s pentagonal shape. Under an electron microscope, CRP looks like five identical subunits arranged in a ring, roughly like five coins fanned into a disc. For history buffs, it resembles the five-star rank worn by General Eisenhower.
Each subunit carries a binding site made of two calcium ions nestled next to a small hydrophobic pocket. This is where CRP does its recognition work: the calcium-dependent sites allow it to grab onto phosphocholine (PC), a molecule found in the membranes of damaged and dying cells, as well as in the outer coatings of many bacteria and fungi. Phosphocholine is so widespread in biology that this single binding chemistry lets CRP respond to an enormous range of threats including microbial invaders and the body’s own dead cells.
CRP doesn’t always exist in this five-subunit ring form. The pentameric version (pCRP) circulates in healthy blood. But at sites of active tissue damage, such as inside an inflamed artery wall, it can break apart into individual monomers (mCRP). These two forms turn out to have strikingly different effects on the immune system.
What CRP Does
It’s tempting to think of CRP as a passive number on a lab report, but it’s actually an active participant in the immune response. It plays at least four major roles.
First, CRP is a pattern recognition molecule. Unlike the antibodies generated by your adaptive immune system which take days or weeks to respond to a specific threat, CRP responds immediately to general molecular patterns shared by pathogens and damaged cells. This makes it a first-responder tool within the innate immune system, the body’s rapid defense network.
Second, once CRP binds to a pathogen or dying cell, it acts as an opsonin, essentially a molecular flag that says “eat this.” Immune cells called phagocytes (macrophages and neutrophils) recognize CRP-coated targets and engulf them, accelerating the clearance of both bacteria and cellular debris.
Third, CRP can activate the complement system, a cascade of proteins that further tags pathogens for destruction. Crucially, CRP appears to stop short of triggering the most destructive steps of that cascade. The net effect is a measured, targeted immune response rather than an all-out inflammatory assault.
Fourth, and this is where things get interesting, the pentameric and monomeric forms of CRP have opposing effects. The pentameric form in circulation is primarily anti-inflammatory, quietly clearing dead cells without triggering unnecessary immune activation. But the monomeric form that appears at sites of tissue damage can amplify inflammation: activating platelets, recruiting immune cells to vessel walls, and stimulating the release of the inflammatory signaling molecule. CRP is neither simply good nor simply bad — it’s context-dependent, functioning as a careful janitor in healthy tissue but potentially fanning the flames in already-inflamed environments.
Fast, Sensitive, and Liver-Made
CRP is produced primarily by liver cells (hepatocytes) in response to immune signals. When immune cells detect infection or tissue damage, they release cytokines, which travel to the liver and switch on CRP production.
One of CRP’s great clinical virtues is speed. Levels can begin rising within four to six hours of an inflammatory event and typically peak within 24 to 48 hours. When the inflammation resolves, CRP falls just as quickly, its half-life in circulation is only about 19 hours. This fast-on, fast-off behavior makes CRP an excellent real-time readout of what the immune system is doing right now, not weeks ago. Because of this early availability, it is referred to as an acute phase reactant.
Under normal, non-inflammatory conditions, CRP in the blood typically measures below 1 milligram per liter (mg/L). During serious bacterial infection or major tissue injury, levels can spike above 400 mg/L — a several-hundred-fold increase. CRP also has a practical advantage for testing: it doesn’t fluctuate throughout the day, and fasting is not required before a blood draw.
The Many Uses of CRP in Clinical Medicine
The oldest application of CRP testing is detecting and monitoring bacterial infection. Very high values — generally above 100 mg/L — strongly suggest bacterial rather than viral infection, since viruses tend to provoke a much more modest CRP rise. In sepsis (the life-threatening systemic response to infection), CRP is one of several markers used to assess severity and track the response to treatment.
CRP is also routinely used to monitor autoimmune diseases. In rheumatoid arthritis, CRP is included in standard disease activity scoring tools. Tracking CRP over time helps clinicians judge whether treatments like disease-modifying drugs are working. One notable exception: in systemic lupus erythematosus (SLE), CRP often stays surprisingly low even during active flares.
Perhaps the most debated expansion of CRP testing in recent decades is its role in cardiovascular risk assessment. That story begins with the recognition that atherosclerosis, the plaque buildup inside artery walls, is fundamentally an inflammatory process, not just a plumbing problem caused by too much cholesterol. As that insight took hold in the 1990s, researchers began asking whether CRP could predict heart attack risk the way cholesterol does.
The answer was yes, but only with a more sensitive test. Standard CRP assays can’t detect levels below about 10 mg/L, which is fine for infections but misses the chronic low-level inflammation relevant to cardiovascular risk. A newer high-sensitivity CRP test (hs-CRP) can measure levels as low as 0.01 mg/L. Using hs-CRP, researchers found that even modest CRP elevations, within the range once considered entirely normal, carry meaningful cardiovascular risk.
The American Heart Association and the CDC use these hs-CRP thresholds for cardiovascular risk: below 1 mg/L is low risk; 1 to 3 mg/L is intermediate risk; above 3 mg/L is higher risk. A large UK Biobank analysis of nearly 450,000 people found that individuals with hs-CRP above 3 mg/L had a 34% higher risk of major cardiovascular events and a 61% higher risk of cardiovascular death compared to those below 1 mg/L.
The landmark JUPITER trial demonstrated that patients with low LDL cholesterol, but elevated hs-CRP (above 2 mg/L) still benefited substantially from statin therapy — in terms of reduced heart attacks and strokes. This reframed how cardiologists think about inflammation as a cardiovascular target independent of cholesterol levels.
Beyond infection, autoimmune disorders, and heart disease, elevated CRP has been linked to type 2 diabetes, metabolic syndrome, chronic kidney disease, COPD, depression, and neurodegenerative diseases, all conditions where chronic low-grade inflammation is increasingly recognized as a contributing factor rather than just a side effect.
Measuring CRP: The Standard Test vs. the High-Sensitivity Test
CRP testing is straightforward, just a standard blood draw, no fasting required. Modern automated lab analyzers make it fast and inexpensive, which explains why it shows up so often in clinical workups.
The standard CRP test is the workhorse for detecting acute infection and monitoring inflammatory flares in hospitalized patients. The hs-CRP test uses more sensitive techniques and is the test used for cardiovascular risk assessment.
Because hs-CRP can fluctuate modestly from day to day, cardiovascular guidelines recommend averaging two measurements taken about two weeks apart. Acute illness, recent injury, or even a hard workout can temporarily elevate hs-CRP and produce a misleading result.
Several factors can push CRP higher independently of the disease in question: obesity, smoking, high blood pressure, metabolic syndrome, low HDL cholesterol, and chronic low-grade infections such as gum disease. Age also gradually raises baseline CRP. On the other side, moderate physical activity, weight loss, and statins are all associated with lower CRP — which partly explains the broader cardiovascular benefits of statin therapy beyond cholesterol reduction.
What CRP Can’t Tell You
For all its usefulness, CRP is a nonspecific marker. A reading of 50 mg/L is consistent with a kidney infection, an autoimmune flare, a recent heart attack, or an abdominal cancer. CRP tells you that inflammation or tissue damage is happening somewhere; it doesn’t tell you where or why. Clinical context including symptoms, medical history, and other lab results, is essential for interpretation.
There’s also a genuine unresolved debate about whether CRP elevation actually causes cardiovascular disease or is simply a marker of underlying inflammatory risk. Animal studies in CRP-deficient or CRP-enhanced models have produced inconsistent results. Mendelian randomization studies in humans, a statistical technique that uses genetic variants to approximate a randomized experiment, have generally not supported CRP as a causal driver of heart disease, suggesting it may be more of a reaction than a root cause.
Finally, hs-CRP testing, despite strong evidence, remains underused in primary care, particularly in primary prevention. The 2024 European Society of Cardiology guidelines for chronic coronary syndromes did recommend assessing hs-CRP in patients with suspected coronary artery disease, which reflects accumulating evidence for its utility, but broader implementation lags behind the science. I have to admit, when I was still in active practice, I was unaware of the role of hs-CRP in primary prevention. At the time, it was generally thought to be of use in secondary prevention—actions taken after an initial event. Be sure and ask your doctor about it.
CRP is, in the end, a remarkably versatile tool — a protein that has been doing immune surveillance since long before medicine had a name for it, and one that continues to find new clinical relevance with each decade of research.
Medical Disclaimer
The information provided in this article is intended for general educational and informational purposes only and does not constitute medical advice. It should not be used as a substitute for professional medical advice, diagnosis, or treatment.
Always seek the guidance of a qualified healthcare provider with any questions you may have regarding a medical condition or treatment. Never disregard professional medical advice or delay seeking it because of something you have read here.
If you are experiencing a medical emergency, call 911 or your local emergency number immediately.
The author of this article is a licensed physician, but the views expressed here are solely those of the author and do not represent the official position of any hospital, health system, or medical organization with which the author may be affiliated.
Image generated by the author using ChatGPT
Sources
The following peer-reviewed and clinical references support this article:
Zhou et al. (2024). C-reactive protein: structure, function, regulation, and role in clinical diseases. Frontiers in Immunology. — https://pmc.ncbi.nlm.nih.gov/articles/PMC11211361/
Agrawal & Wu (2024). Editorial: Biology of C-reactive protein. Frontiers in Immunology. — https://www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2024.1445001/full
Volanakis (2001). Human C-reactive protein: expression, structure, and function. Molecular Immunology. PubMed. — https://pubmed.ncbi.nlm.nih.gov/11532280/
Thompson et al. (2004). C-reactive protein. Journal of Biological Chemistry. — https://www.jbc.org/article/S0021-9258(19)32228-8/fulltext
Salazar et al. (2014). C-Reactive Protein: An In-Depth Look into Structure, Function, and Regulation. International Scholarly Research Notices. PMC. — https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4897210/
StatPearls: C-Reactive Protein: Clinical Relevance and Interpretation. PubMed. — https://pubmed.ncbi.nlm.nih.gov/28722873/
Medscape: High-Sensitivity C-Reactive Protein: Reference Range, Interpretation. — https://emedicine.medscape.com/article/2094831-overview
Ridker PM (2003). High-sensitivity C-reactive protein: clinical importance. PubMed. — https://pubmed.ncbi.nlm.nih.gov/15258556/
Kraaijenhof et al. (2025). LDL cholesterol, CRP, and lipoprotein(a) universal screening. European Heart Journal. ACC summary. — https://www.acc.org/latest-in-cardiology/articles/2025/12/01/01/prioritizing-health-hscrp
Johns Hopkins Medicine: Assessing Cardiovascular Risk with C-Reactive Protein. — https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/assessing-cardiovascular-risk-with-c-reactive-protein
Labcorp: C-Reactive Protein (CRP), High Sensitivity (Cardiac Risk Assessment). — https://www.labcorp.com/tests/120766/c-reactive-protein-crp-high-sensitivity-cardiac-risk-assessment
Larsen et al. (2024). C-reactive protein and cardiovascular risk in the general population. European Heart Journal. — https://academic.oup.com/eurheartj/advance-article/doi/10.1093/eurheartj/ehaf937/8377304
Shetty & Kawaguchi (2024). Role of CRP in disease progression, diagnosis and management. PMC. — https://pmc.ncbi.nlm.nih.gov/articles/PMC11569793/
McDonnell et al. (2024). C-reactive protein complement-ary structures in RA. Elsevier/Immunology Letters. — https://www.binasss.sa.cr/ago24/21.pdf
CRP kinetics as predictor in immune checkpoint inhibitor therapy. BJC Reports / Nature. — https://www.nature.com/articles/s44276-023-00005-x
Borges et al. (2024). Battle of the Biomarkers of Systemic Inflammation (CRP vs cfDNA). PMC. — https://pmc.ncbi.nlm.nih.gov/articles/PMC12024891/
Assay Genie: C-reactive protein — structure and function overview. — https://www.assaygenie.com/blog/c-reactive-protein
WebMD: C-Reactive Protein Test: High vs. Low Levels. — https://www.webmd.com/a-to-z-guides/c-reactive-protein-test
Mayo Clinic: C-reactive protein test. —https://www.mayoclinic.org/tests-procedures/c-reactive-protein-test/about/pac-20385228