
Creating a safe home environment becomes increasingly important as we age. Here’s a comprehensive checklist organized by key areas to help seniors and their families identify potential hazards and make practical improvements.
Fall Prevention (General)
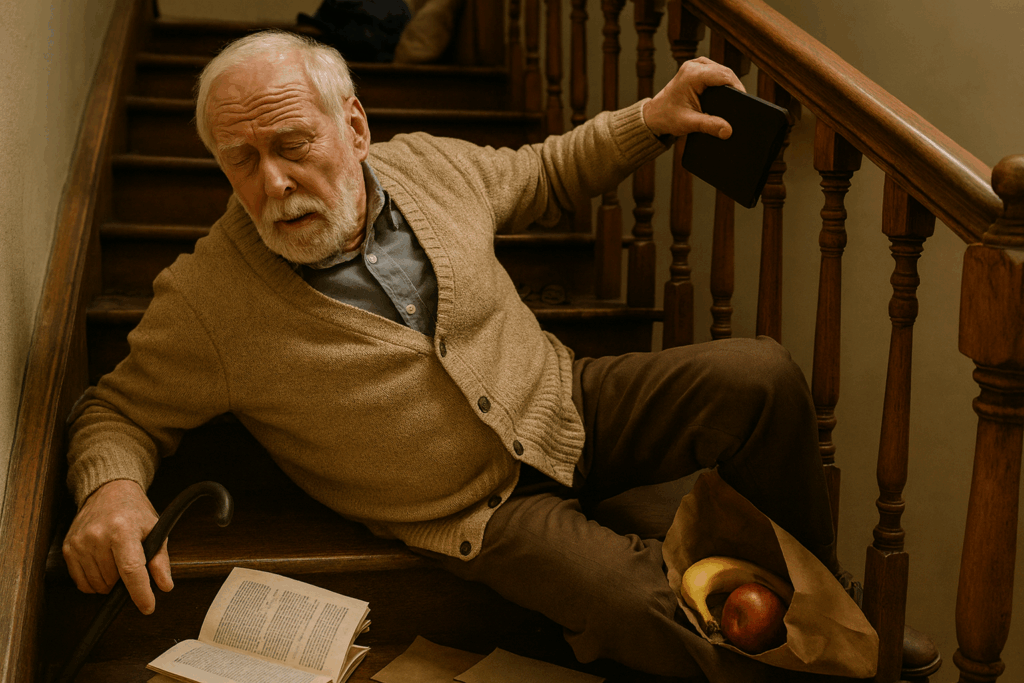
Falls are the leading cause of injury among older adults, accounting for over 3 million emergency department visits annually. Here’s what to address:
- Remove or secure loose rugs and runners throughout the home
- Eliminate clutter from walkways and stairs
- Ensure all stairways have sturdy handrails on both sides
- Improve lighting in all areas, especially hallways and stairways
- Keep frequently used items within easy reach to avoid overreaching
- Repair loose floorboards or uneven flooring
- Use non-slip mats under area rugs
- Arrange furniture to create clear walking paths
- Keep electrical and phone cords away from walking areas
- Use chairs with arms for easier standing
- Wear sturdy, non-slip footwear indoors
Bathroom Safety
The bathroom presents unique challenges due to wet surfaces and the need to transition between sitting and standing positions.
- Install grab bars near the toilet and inside the shower or tub
- Ensure grab bars are mounted directly into wall studs not drywall anchors
- Use suction cup bars only for balance—they will not support your weight
- Use a non-slip bath mat both inside and outside the tub or shower
- Consider a shower chair or tub transfer bench for bathing
- Install a raised toilet seat if needed
- Ensure the bathroom has bright, even lighting
- Keep a nightlight on for nighttime bathroom visits
- Store toiletries within easy reach to avoid stretching
- Set water heater to 120°F or below to prevent scalding
- Consider replacing traditional tub with a walk-in shower
Kitchen Safety
The kitchen involves both fall risks and burn hazards that need attention.
- Store heavy items at waist level to avoid bending or reaching
- Use a sturdy step stool with handrails if reaching is necessary—never use chairs
- Keep a fire extinguisher accessible and ensure it’s up to date
- Wear short or close-fitting sleeves while cooking
- Turn pot handles inward to prevent knocking them over
- Clean up spills immediately to prevent slips
- Ensure adequate lighting over work areas
- Mark “on” and “off” positions clearly on appliance controls
- Consider replacing gas stoves with electric if memory issues are present
Bedroom Safety
Since we spend significant time in the bedroom, it should be optimized for safe movement, especially at night.
- Position the bed at an appropriate height for easy getting in and out
- Keep a lamp or light switch within reach of the bed
- Install nightlights along the path from bedroom to bathroom
- Keep a phone or medical alert device within reach
- Ensure smoke and carbon monoxide detectors are installed and functional
- Avoid placing electrical cords near the bed where they could cause tripping
- Use a firm mattress that provides adequate support
- Keep a flashlight on the nightstand in case of power outages
- Position cane or walker within easy reach if needed
Lighting Throughout the Home
Poor lighting significantly increases fall risk, yet it’s one of the easiest issues to address.
- Increase wattage in existing fixtures (within safe limits)
- Add lighting to dark hallways, stairways, and entrances
- Install motion-sensor lights for convenience
- Use nightlights in bathrooms, hallways, and bedrooms
- Ensure light switches are accessible at room entrances
- Replace burnt-out bulbs promptly
- Consider adding illuminated light switches
- Ensure outdoor entrances are well-lit
Stairway Safety
Stairs are high-risk areas that deserve special attention and modifications.
- Ensure handrails extend the full length of stairs
- Mark the edge of each step with bright, contrasting tape if not carpeted
- Repair any loose steps or carpeting immediately
- Ensure adequate lighting with switches at both top and bottom
- Avoid storing items on stairs
- Consider installing a stair lift if mobility is significantly impaired
- Keep exterior stairs clear of ice and snow in winter
Fire and Emergency Safety
Quick response to emergencies can be lifesaving, so preparation is essential.
- Install smoke detectors on every level and in each bedroom
- Test smoke and carbon monoxide detectors monthly
- Replace detector batteries at least annually
- Keep fire extinguishers accessible in kitchen and garage
- Create and practice an emergency exit plan
- Post emergency numbers near all phones
- Ensure house numbers are visible from the street for emergency responders
- Consider a medical alert system, especially for those living alone
- Keep a phone accessible at all times
Medication Safety
Medication management becomes more complex with age, and organization is key.
- Use a pill organizer to track daily medications
- Keep medications in original containers with clear labels
- Store medications in a cool, dry place (not the bathroom)
- Maintain an updated list of all medications and dosages
- Discard expired medications properly
- Ensure adequate lighting in areas where medications are taken
- Set reminders for medication times
- Consider a medication app for your smart phone
- Keep a medication list in your wallet for emergencies
Technology and Communication
Staying connected improves both safety and quality of life.
- Keep a charged cell phone accessible at all times
- Consider a medical alert system with fall detection
- Program emergency contacts into phones
- Ensure phones have large buttons and clear displays if vision is impaired
- Keep a list of emergency contacts posted in visible locations
- Consider smart home devices that can control lights and temperature by voice
Outdoor Safety
The area outside the home also requires attention to prevent falls and injuries.
- Repair cracked or uneven walkways and driveways
- Ensure outdoor steps have sturdy handrails
- Keep walkways clear of leaves, ice, and snow
- Trim overgrown bushes and trees that obstruct paths
- Ensure outdoor lighting is adequate for evening and early morning
- Use non-slip materials on outdoor steps
- Consider replacing steps with ramps if mobility is significantly limited
- Place nonslip mats outside entry doors to reduce tracking in moisture or mud
This checklist is based on well-established safety guidelines from organizations like the CDC and National Fire Protection Association. The specific recommendations reflect current best practices in senior home safety. However, individual needs vary significantly based on specific mobility issues, health conditions, and home layouts, so some modifications may be more relevant than others for different situations.
Note: While these recommendations are widely applicable, it’s beneficial to have an occupational therapist or home safety specialist conduct a personalized assessment, as they can identify specific risks based on individual circumstances and home characteristics.










No Kings!
By John Turley
On October 18, 2025
In Commentary, Politics