The mythology of the founding fathers often portrays them as a harmonious band of brothers united in noble purpose. The reality was far messier—these brilliant, ambitious men engaged in bitter personal feuds that sometimes threatened the very republic they were creating. In some ways, the American revolution was as much of a battle of egos as it was a war between King and colonists.
The Revolutionary War Years: Hancock, Adams, and Washington’s Critics
The tensions began even before independence was declared. John Hancock and Samuel Adams, both Massachusetts firebrands, developed a rivalry that simmered throughout the Revolution. Adams, the older political strategist, had been the dominant figure in Boston’s resistance movement. When Hancock—wealthy, vain, and eager for glory—was elected president of the Continental Congress in 1775, the austere Adams felt his protégé had grown too big for his britches. Hancock’s request for a leave of absence from the presidency of Congress in 1777 coupled with his desire for an honorific military escort home, struck Adams as a relapse into vanity. Adams even opposed a resolution of thanks for Hancock’s service, signaling open estrangement. Their relationship continued to deteriorate to the point where they barely spoke, with Adams privately mocking Hancock’s pretensions and Hancock using his position to undercut Adams politically.
The choice of Washington as commander sparked its own controversies. John Adams had nominated Washington, partly to unite the colonies by giving Virginia the top military role. Washington’s command was anything but universally admired and as the war dragged on with mixed results many critics emerged.
After the victory at Saratoga in 1777, General Horatio Gates became the focal point of what’s known as the Conway Cabal—a loose conspiracy aimed at having Gates replace Washington as commander-in-chief. General Thomas Conway wrote disparaging letters about Washington’s military abilities. Some members of Congress, including Samuel Adams, Thomas Mifflin, and Richard Henry Lee, questioned whether Washington’s defensive strategy was too cautious and if his battlefield performance was lacking. Gates himself played a duplicitous game, publicly supporting Washington while privately positioning himself as an alternative.
When Washington discovered the intrigue, his response was characteristically measured but firm. Rather than lobbying Congress or forming a counter-faction, Washington leaned heavily on reputation and restraint. He continued to communicate respectfully with Congress, emphasizing the army’s needs rather than defending his own position. Washington did not respond with denunciations or public accusations. Instead, he handled the situation largely behind the scenes. When he learned that Conway had written a critical letter praising Gates, Washington calmly informed him that he was aware of the letter—quoting it verbatim.
The conspiracy collapsed, in part because Washington’s personal reputation with the rank and file and with key political figures proved more resilient than his critics had anticipated. But the episode exposed deep fractures over strategy, leadership, and regional loyalties within the revolutionary coalition.
The Ideological Split: Hamilton vs. Jefferson and Madison
Perhaps the most consequential feud emerged in the 1790s between Alexander Hamilton and Thomas Jefferson, with James Madison eventually siding with Jefferson. This wasn’t just personal animosity—it represented a fundamental disagreement about America’s future.
Hamilton, Washington’s Treasury Secretary, envisioned an industrialized commercial nation with a strong central government, a national bank, and close ties to Britain. Jefferson, the Secretary of State, championed an agrarian republic of small farmers with minimal federal power and friendship with Revolutionary France. Their cabinet meetings became so contentious that Washington had to mediate. Hamilton accused Jefferson of being a dangerous radical who would destroy public credit. Jefferson called Hamilton a monarchist who wanted to recreate British aristocracy in America.
The conflict got personal. Hamilton leaked damaging information about Jefferson to friendly newspapers. Jefferson secretly funded a journalist, James Callender, to attack Hamilton in print. When Hamilton’s extramarital affair with Maria Reynolds became public in 1797, Jefferson’s allies savored every detail. The feud split the nation into the first political parties: Hamilton’s Federalists and Jefferson’s Democratic-Republicans. Madison, once Hamilton’s ally in promoting the Constitution, switched sides completely, becoming Jefferson’s closest political partner and Hamilton’s implacable foe.
The Adams-Jefferson Friendship, Rivalry, and Reconciliation
John Adams and Thomas Jefferson experienced one of history’s most remarkable personal relationships. They were close friends during the Revolution, working together in Congress and on the committee to draft the Declaration of Independence (though Jefferson did the actual writing). Both served diplomatic posts in Europe and developed deep mutual respect.
But the election of 1796 turned them into rivals. Adams won the presidency with Jefferson finishing second, making Jefferson vice president under the original constitutional system—imagine your closest competitor becoming your deputy. By the 1800 election, they were bitter enemies. The campaign was vicious, with Jefferson’s supporters calling Adams a “hideous hermaphroditical character” and Adams’s allies claiming Jefferson was an atheist who would destroy Christianity.
Jefferson won in 1800, and the two men didn’t speak for over a decade. Their relationship was so bitter that Adams left Washington early in the morning, before Jefferson’s inauguration. What makes their story extraordinary is the reconciliation. In 1812, mutual friends convinced them to resume correspondence. Their letters over the next fourteen years—158 of them—became one of the great intellectual exchanges in American history, discussing philosophy, politics, and their memories of the Revolution. Both men died on July 4, 1826, the fiftieth anniversary of the Declaration of Independence, with Adams’s last words reportedly being “Thomas Jefferson survives” (though Jefferson had actually died hours earlier).
Franklin vs. Adams: A Clash of Styles
In Paris, the relationship between Benjamin Franklin and John Adams was a tense blend of grudging professional reliance and deep personal irritation, rooted in radically different diplomatic styles and temperaments. Franklin, already a celebrated figure at Versailles, cultivated French support through charm, sociability, and patient maneuvering in salons and at court, a method that infuriated Adams. He equated such “nuances” with evasiveness and preferred direct argument, formal memorandums, and hard‑edged ultimatums. Sharing lodgings outside Paris only intensified Adams’s resentment as he watched Franklin rise late, receive endless visitors, and seemingly mix pleasure with business, leading Adams to complain that nothing would ever get done unless he did it himself, while Franklin privately judged Adams “always an honest man, often a wise one, but sometimes and in some things, absolutely out of his senses.” Their French ally, Foreign Minister Vergennes, reinforced the imbalance by insisting on dealing primarily with Franklin and effectively sidelining Adams in formal diplomacy. This deepened Adams’s sense that Franklin was both overindulged by the French and insufficiently assertive on America’s behalf. Yet despite their mutual loss of respect, the two ultimately cooperated—often uneasily—in the peace negotiations with Britain, and both signatures appear on the 1783 Treaty of Paris, a testament to the way personal feud and shared national purpose coexisted within the American diplomatic mission.
Hamilton and Burr: From Political Rivalry to Fatal Duel
The Hamilton-Burr feud ended in the most dramatic way possible: a duel at Weehawken, New Jersey, on July 11, 1804, where Hamilton was mortally wounded and Burr destroyed his own political career.
Their rivalry had been building for years. Both were New York lawyers and politicians, but Hamilton consistently blocked Burr’s ambitions. When Burr ran for governor of New York in 1804, Hamilton campaigned against him with particular venom, calling Burr dangerous and untrustworthy at a dinner party. When Burr read accounts of Hamilton’s remarks in a newspaper, he demanded an apology. Hamilton refused to apologize or deny the comments, leading to the duel challenge.
What made this especially tragic was that Hamilton’s oldest son, Philip, had been killed in a duel three years earlier defending his father’s honor. Hamilton reportedly planned to withhold his fire, but he either intentionally shot into the air or missed. Burr’s shot struck Hamilton in the abdomen, and he died the next day. Burr was charged with murder in both New York and New Jersey and fled to the South. Though he later returned to complete his term as vice president, his political career was finished.
Adams vs. Hamilton: The Federalist Crack-Up
One of the most destructive feuds happened within the same party. John Adams and Alexander Hamilton were both Federalists, but their relationship became poisonous during Adams’s presidency (1797-1801).
Hamilton, though not in government, tried to control Adams’s cabinet from behind the scenes. When Adams pursued peace negotiations with France (the “Quasi-War” with France was raging), Hamilton wanted war. Adams discovered that several of his cabinet members were more loyal to Hamilton than to him and fired them. In the 1800 election, Hamilton wrote a fifty-four-page pamphlet attacking Adams’s character and fitness for office—extraordinary since they were in the same party. The pamphlet was meant for limited circulation among Federalist leaders, but Jefferson’s allies got hold of it and published it widely, devastating both Adams’s re-election chances and Hamilton’s reputation. The feud helped Jefferson win and essentially destroyed the Federalist Party.
Washington and Jefferson: The Unacknowledged Tension
While Washington and Jefferson never had an open feud, their relationship cooled significantly during Washington’s presidency. Jefferson, as Secretary of State, increasingly opposed the administration’s policies, particularly Hamilton’s financial program. When Washington supported the Jay Treaty with Britain in 1795—which Jefferson saw as a betrayal of France and Republican principles—Jefferson became convinced Washington had fallen under Hamilton’s spell.
Jefferson resigned from the cabinet in 1793, partly from policy disagreements but also from discomfort with what he saw as Washington’s monarchical tendencies (the formal receptions and the ceremonial aspects of the presidency). Washington, in turn, came to view Jefferson as disloyal, especially when he learned Jefferson had been secretly funding attacks on the administration in opposition newspapers and had even put a leading critic on the federal payroll. By the time Washington delivered his Farewell Address in 1796, warning against political parties and foreign entanglements, many saw it as a rebuke of Jefferson’s philosophy. They maintained outward courtesy, but their warm relationship never recovered.
Why These Feuds Mattered
These weren’t just personal squabbles—they shaped American democracy in profound ways. The Hamilton-Jefferson rivalry created our two-party system (despite Washington’s warnings). The Adams-Hamilton split showed that parties could fracture from within. The Adams-Jefferson reconciliation demonstrated that political enemies could find common ground after leaving power.
The founding fathers were human, with all the ambition, pride, jealousy, and pettiness that entails. They fought over power, principles, and personal slights. What’s remarkable isn’t that they agreed on everything—they clearly didn’t—but that despite their bitter divisions, they created a system robust enough to survive their feuds. The Constitution itself, with its checks and balances, almost seems designed to accommodate such disagreements, ensuring that no single person or faction could dominate.
SOURCES
- National Archives – Founders Online
https://founders.archives.gov
2. Massachusetts Historical Society – Adams-Jefferson Letters
https://www.masshist.org/publications/adams-jefferson
3. Founders Online – Hamilton’s Letter Concerning John Adams
https://founders.archives.gov/documents/Hamilton/01-25-02-0110
4. Gilder Lehrman Institute – Hamilton and Jefferson
https://www.gilderlehrman.org/history-resources/spotlight-primary-source/alexander-hamilton-and-thomas-jefferson
5. National Park Service – The Conway Cabal
https://www.nps.gov/articles/000/the-conway-cabal.htm
6. American Battlefield Trust – Hamilton-Burr Duel
https://www.battlefields.org/learn/articles/hamilton-burr-duel
7. Mount Vernon – Thomas Jefferson
https://www.mountvernon.org/library/digitalhistory/digital-encyclopedia/article/thomas-jefferson
8. Monticello – Thomas Jefferson Encyclopedia
https://www.monticello.org/research-education/thomas-jefferson-encyclopedia
9. Library of Congress – John Adams Papers
https://www.loc.gov/collections/john-adams-papers
10. Joseph Ellis – “Founding Brothers: The Revolutionary Generation”
https://www.pulitzer.org/winners/joseph-j-ellis
Illustration generated by author using ChatGPT.







The Accidental Footnote: Heel Spurs, the Vietnam Draft, and American Inequality
By John Turley
On April 17, 2026
In Commentary, History, Medicine, Politics
If you’ve ever winced taking your first steps out of bed in the morning, you may have already made an involuntary acquaintance with heel spurs — or more precisely, with the condition that often travels with them. The term itself sounds alarming, and for a brief but colorful stretch of American political history, it became something far more charged than a footnote to podiatry. But before we get to the politics, it’s worth understanding what a heel spur actually is, because the medical reality is both more mundane and more complicated than the caricature.
What Exactly Is a Heel Spur?
A heel spur is a small bony outgrowth — technically called a calcaneal spur — that extends from the underside of the heel bone (the calcaneus). It forms at the spot where the plantar fascia — the thick ligament running the length of your foot from heel to toe — attaches to the heel bone. The spur is not, despite what the name implies, a sharp spike. It is typically smooth and rounded, though it can still cause irritation if it presses into surrounding soft tissue.
Heel spurs affect about 10% of the population, making them one of the more common foot conditions around, though most people who have one don’t know it. The spur develops gradually — usually over months or even years — as the body deposits calcium in response to chronic stress at that heel attachment point. Think of it less as damage and more as your skeleton’s attempt at reinforcement.
What Causes Them?
The underlying driver is repetitive mechanical stress on the foot. Heel spurs are particularly associated with strains on foot muscles and ligaments, stretching of the plantar fascia, and repeated small tears in the membrane covering the heel bone. Athletes who do a lot of running and jumping are especially prone.
But you don’t need to be an elite runner to develop one. Walking gait problems — particularly overpronation, where the foot rolls inward — place uneven stress on the heel with each step. Worn-out or poorly fitted shoes, which fail to absorb shock or support the arch, compound the problem. Obesity increases the mechanical load on the heel. Occupations that require prolonged standing or walking on hard surfaces put the plantar fascia under constant tension. And as people age, tendons and ligaments lose their elasticity, making the tissues more vulnerable to micro-tears and the subsequent bony repair response.
Heel spurs are also closely connected to a condition most people have heard of: plantar fasciitis. The two are related a but not identical. Plantar fasciitis is inflammation of the plantar fascia itself, usually from overuse. A heel spur can develop as a downstream consequence of that inflammation — the body lays down extra bone in response to the ongoing stress at the fascia’s attachment point.
Symptoms — or the Lack Thereof
Here’s the part that surprises most people: the majority of heel spurs cause no symptoms at all, and many are discovered incidentally on X-rays taken for other reasons. Only about 5% of heel spurs are estimated to be symptomatic.
When a heel spur does produce symptoms, the experience is heavily intertwined with plantar fasciitis. The classic description is a sharp, stabbing pain on the bottom of the foot first thing in the morning, or after any prolonged rest. Many people compare it to stepping on a tack. Paradoxically, this pain often eases somewhat after walking around for a few minutes, only to return after extended time on the feet or after another rest. It’s that “worse in the morning” quality that tends to be the giveaway.
Other symptoms, when present, can include localized swelling, warmth, and tenderness along the front of the heel, as well as increased sensitivity on the underside of the foot. It’s worth noting that the pain associated with a heel spur is not generally thought to come from the bony spur itself, but from the irritation it causes in the surrounding soft tissue — tendons, ligaments, and bursae.
How Is It Diagnosed?
Diagnosis typically begins with a physical exam. Your doctor or podiatrist will ask about when the pain started, what activities preceded it, and what makes it better or worse. They’ll examine your foot for tenderness at specific points, assess your range of motion, and check foot alignment and press on key areas to locate the source of pain.
Imaging confirms the picture. An X-ray can clearly show the bony spur and is the most commonly used test. That said, the size of the spur on an X-ray doesn’t necessarily correspond to how much pain a patient is experiencing — a small spur can be quite painful while a large one may cause no trouble at all. In more complex cases, an MRI may be ordered to assess the soft tissues more closely and evaluate whether plantar fasciitis or another condition is also in play.
Treatment Options
The reassuring news is that the vast majority of cases resolve without surgery. More than 90% of patients improve with nonsurgical treatment. The catch is that conservative management requires patience — improvement typically takes weeks, and more stubborn cases can take months.
The cornerstone of treatment is rest and reducing the activities that provoke pain. This doesn’t necessarily mean completely stopping exercise; low-impact alternatives like swimming, cycling, or rowing allow you to stay active while giving the heel a break from impact. Icing the bottom of the foot after activity helps manage inflammation. Over-the-counter anti-inflammatory medications like ibuprofen or naproxen can provide relief, though they’re intended for short-term use.
Footwear matters enormously. Supportive shoes with good arch support, cushioning, and a slight heel rise reduce the strain on the plantar fascia. Custom orthotics with molded insoles designed to redistribute pressure across the foot are often recommended, particularly for people with gait abnormalities or flat feet. Physical therapy can be part of the treatment plan, focusing on stretching the calf muscles and plantar fascia, strengthening the foot’s intrinsic muscles, and correcting biomechanical issues.
For cases that don’t respond to these initial measures, the next tier of treatment includes corticosteroid injections to reduce inflammation at the spur site, and extracorporeal shockwave therapy — a non-invasive procedure that uses sound waves to stimulate healing in chronically inflamed tissue. Surgery is reserved for the minority of cases where conservative treatment fails after nine to twelve months. Possible complications include nerve pain, infection, scarring, and — with plantar fascia release — the risk of foot instability or stress fracture. Most orthopedic surgeons regard surgery as a last resort.
Are Heel Spurs Debilitating?
For most people, the honest answer is: no. Heel spurs are a common condition with a favorable prognosis, especially with early diagnosis and appropriate management. Many people live with heel spurs for years without ever knowing it, and even those who develop pain typically find substantial relief with conservative treatment within four to eight weeks.
That said, the pain at its worst — particularly in conjunction with plantar fasciitis — can be genuinely disruptive to daily life. Athletes may find their training significantly limited. People who spend long hours on their feet at work may struggle with sustained discomfort. And a small percentage of patients do end up with prolonged, treatment-resistant pain that affects mobility. So, the more accurate framing might be: heel spurs have the potential to be significantly uncomfortable and functionally limiting during flare-ups, but with proper treatment most people recover well and return to normal activity.
Heel Spurs and the Vietnam-Era Draft
Which brings us to an improbable chapter in heel spur history. During the Vietnam War era, heel spurs became — for at least one famous case — a ticket out of military service. Understanding how that worked requires a brief detour into the draft system of the 1960s and 1970s, and what it meant to receive a medical deferment.
According to the National Archives, of the roughly 27 million American men eligible for military service between 1964 and 1973, about 15 million were granted deferments — mostly for education, and some for mental or physical problems — while only 2,215,000 were actually drafted into service—another eight million volunteered. Some of those who later served had previously had deferments. The system was sprawling, complex, and — as was widely acknowledged even at the time — deeply unequal.
Roughly 60% of draft-eligible American men took some sort of action to avoid military conscription. There were many routes: college deferments, fatherhood, conscientious objector status (170,000 men received those alone), National Guard enlistment, and medical exemptions. Medical deferments covered a wide range of conditions — from serious chronic illness to conditions that, in a different context, most people would consider minor. Flat feet, poor eyesight, asthma, and yes, bone spurs all appeared on the list of potentially disqualifying ailments.
The system was known to favor men with access to money, education, and well-connected physicians. American forces in Vietnam were 55% working-class and 25% poor — reflecting those who didn’t have the means to navigate the deferment labyrinth. A working-class kid from rural West Virginia was far more likely to end up in the Mekong Delta than the son of a New York real estate developer.
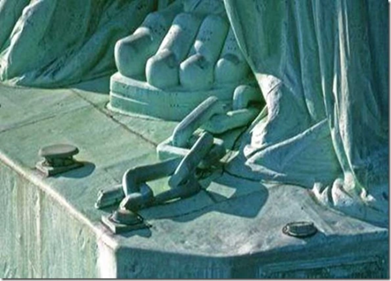
The Most Famous Heel Spur in American History
Which leads, inevitably, to Donald Trump. As confirmed by Selective Service records obtained and reported by multiple news outlets, Trump received five Vietnam-era draft deferments — four for college attendance at Fordham and the Wharton School, and a fifth in 1968, recorded as a medical deferment for bone spurs in his heels. The medical classification left him disqualified for military service.
The circumstances surrounding the diagnosis have been contested ever since. Reporting by the New York Times included accounts from the daughters of a Queens podiatrist named Larry Braunstein, who alleged that their father had provided or vouched for the diagnosis as a professional favor to Trump’s father, Fred Trump — a landlord to whom Braunstein reportedly owed a debt of gratitude. Trump’s former lawyer Michael Cohen also testified that Trump had admitted to fabricating the injury. Trump himself has maintained that the diagnosis was legitimate, stating that a doctor “gave me a letter — a very strong letter — on the heels.” The underlying medical records that would resolve the dispute are, conveniently, not publicly available; most individual Selective Service medical records from that era were subsequently destroyed.
It’s worth noting that Trump’s pattern — using legal channels, including a medical deferment of questionable validity, to avoid Vietnam service — was not unique to him. Historians have pointed out that numerous prominent figures on both sides of the political aisle received deferments of various kinds, including Joe Biden (asthma), Dick Cheney (student deferments), Bill Clinton (navigated the ROTC system), and George W. Bush (National Guard). The heel spur episode became politically charged in part because of Trump’s later hawkish rhetoric and his outspokenness in questioning the military service of others — most notably Senator John McCain, who spent years as a prisoner of war in North Vietnam.
How Many People Got Heel Spur Deferments?
This is where the historical record hits a hard wall. No reliable statistics exist specifically for heel spur deferments. The Selective Service tracked broad categories — student deferments, hardship deferments, conscientious objector status, medical disqualifications — but it did not publish a breakdown by specific diagnosis, and most individual medical records from that era no longer exist.
What we can say is that bone spurs were a recognized medical disqualifier under Selective Service regulations, that medical deferments broadly were a commonly used — and commonly abused — avenue for avoiding service, and that the process was heavily influenced by access to sympathetic physicians. A man with means, connections, and a cooperative podiatrist had options that a man without those resources did not.
The honest answer, then, is that we don’t know how many men received deferments citing heel spurs specifically, and we almost certainly never will. The data either wasn’t tracked at that level of granularity or was long since destroyed. What we do know is that the condition became, for a time, a lens through which Americans examined something much larger: who serves, who doesn’t, and whether the systems meant to govern those decisions are applied fairly.
For most people, a heel spur is a manageable, if annoying, footnote in the story of their health. For at least one person, it became a footnote in the history of American politics.
Personal Note: I have heel spurs; I wish I’d known about them in 1967.
Images generated by author using AI.
Medical Sources
Cleveland Clinic — Heel Spurs overview
https://my.clevelandclinic.org/health/diseases/21965-heel-spurs
WebMD — Heel Spur Causes, Symptoms, Treatments, and Surgery
https://www.webmd.com/pain-management/heel-spurs-pain-causes-symptoms-treatments
Hackensack Meridian Health — Bone Spurs in the Heel: Symptoms and Recovery
https://www.hackensackmeridianhealth.org/en/healthier-you/2024/01/02/bone-spurs-in-the-heel-symptoms-and-recovery
OrthoArkansas — Heel Spurs
https://www.orthoarkansas.com/heel-spurs-orthoarkansas/
EmergeOrtho — Heel Bone Spurs: Causes, Symptoms, Treatment
https://emergeortho.com/news/heel-bone-spurs/
American Academy of Orthopaedic Surgeons — Plantar Fasciitis and Bone Spurs
https://orthoinfo.aaos.org/en/diseases–conditions/plantar-fasciitis-and-bone-spurs/
Vietnam Draft & Military Service Sources
History.com — 7 Ways Americans Avoided the Draft During the Vietnam War
https://www.history.com/articles/vietnam-war-draft-avoiding
Wikipedia — Draft Evasion in the Vietnam War
https://en.wikipedia.org/wiki/Draft_evasion_in_the_Vietnam_War
Wikipedia — Conscription in the United States
https://en.wikipedia.org/wiki/Conscription_in_the_United_States
Students of History — The Draft and the Vietnam War
https://www.studentsofhistory.com/vietnam-war-draft
University of Michigan — The Military Draft During the Vietnam War
https://michiganintheworld.history.lsa.umich.edu/antivietnamwar/exhibits/show/exhibit/draft_protests/the-military-draft-during-the-
Vietnam Veterans of America Chapter 310 — Vietnam War Statistics
https://www.vva310.org/vietnam-war-statistics
Vietnam Veterans of Foreign Wars — Fact vs. Fiction: The Vietnam Veteran
https://www.vvof.org/factsvnv.htm
New York City Vietnam Veterans Plaza — Interesting Facts About Vietnam
https://www.vietnamveteransplaza.com/interesting-facts-about-vietnam/
Medical Disclaimer
The information provided in this article is intended for general educational and informational purposes only and does not constitute medical advice. It should not be used as a substitute for professional medical advice, diagnosis, or treatment.
Always seek the guidance of a qualified healthcare provider with any questions you may have regarding a medical condition or treatment. Never disregard professional medical advice or delay seeking it because of something you have read here.
If you are experiencing a medical emergency, call 911 or your local emergency number immediately.
The author of this article is a licensed physician, but the views expressed here are solely those of the author and do not represent the official position of any hospital, health system, or medical organization with which the author may be affiliated.