
Chronic kidney disease (CKD) affects approximately 37 million Americans, with adults over 65 representing the fastest-growing group diagnosed. Often called a “silent disease,” CKD can progress for years without noticeable symptoms, making awareness and early detection crucial for preserving kidney function and overall health.
What Is Chronic Kidney Disease?
Chronic kidney disease occurs when the kidneys gradually lose their ability to filter waste products and excess fluid from the blood. Unlike acute kidney injury, which happens suddenly and can be quickly corrected, CKD develops slowly over months or years and is generally not reversable. The kidneys perform several vital functions beyond filtration, including regulating blood pressure, supporting production of red blood cells, and maintaining the body’s chemical balance. When kidney function declines, these processes become compromised, leading to serious health complications if left untreated.
The disease progresses through five stages, from mild kidney damage with normal filtration to complete kidney failure requiring dialysis or transplantation. Understanding this progression helps patients and healthcare providers make informed decisions about treatment and lifestyle modifications.
Risk Factors: Who’s Most Vulnerable?
Several factors significantly increase the risk of developing CKD, with diabetes and high blood pressure being the leading causes and accounting for nearly two-thirds of all cases.
Type 2 diabetes, which affects over 11% of the U.S. population, damages the small blood vessels in the kidneys impairing their filtering capacity. Kidneys also play a role in glucose management by clearing insulin from the body. As kidney function declines, insulin stays in the system longer reducing circulating glucose levels.
Hypertension creates a destructive cycle of progressive kidney disease. It damages kidney blood vessels, reducing their effectiveness, causing the kidneys to struggle to regulate blood pressure, creating further blood pressure elevation, leading to greater damage. This relationship makes blood pressure control essential for both prevention and treatment.
Age itself is a significant risk factor. After age 40, kidney function naturally declines by approximately 1% per year. However, this normal aging process can accelerate in the presence of other risk factors. Family history also plays a role, particularly for conditions like polycystic kidney disease and certain genetic disorders affecting kidney function.
Other risk factors include cardiovascular disease, obesity, smoking, and prolonged use of certain medications, particularly nonsteroidal anti-inflammatory drugs (NSAID—aspirin, ibuprofen, etc) and some prescription medications. African Americans, Hispanic Americans, and Native Americans face higher risks due to genetic predisposition and higher rates of diabetes and hypertension. As with all chronic medical conditions, the detrimental effect of smoking cannot be overstated.
Recognizing the Signs: Symptoms of CKD
The insidious nature of CKD means symptoms often don’t appear until after significant kidney damage has occurred. Early-stage CKD may produce no symptoms at all, which is why routine screening for at-risk individuals is so important.
As the disease progresses, symptoms may include persistent fatigue and weakness which are often dismissed as normal aging. Patients may have trouble concentrating, sleep problems, decreased appetite and persistent nausea. Swelling in the feet, ankles, or around the eyes can indicate fluid retention due to impaired kidney function.
Changes in urination patterns may occur, including increased frequency, especially at night, or decreased urine output. The urine may appear foamy, indicating protein spillage, or may be darker in color. Some patients experience persistent itching due to waste product buildup in the blood.
More advanced CKD can cause severe nausea, vomiting, muscle cramps, and shortness of breath. High blood pressure may develop or worsen, and patients might experience chest pain or irregular heartbeats. These symptoms warrant immediate medical attention.
Diagnostic Testing: Identifying CKD
Early detection relies on simple, routine blood and urine tests that can identify kidney problems before symptoms appear. Your doctor will order blood tests and urine tests, and possibly imaging tests such as ultrasounds to evaluate your risk for kidney disease. Frequently these tests will check for many other things such as anemia, high cholesterol or diabetes. All of these can contribute to chronic kidney disease.
Treatment Approaches: Managing CKD
While CKD cannot be cured, proper treatment can significantly slow progression and manage complications. The primary goals include treating underlying causes, slowing decline of kidney function, and managing associated health problems.
Blood pressure control is paramount, with target levels typically below 130/80 mmHg for most CKD patients. ACE inhibitors and ARBs (angiotensin receptor blockers) are preferred medications as they provide additional kidney protection beyond blood pressure reduction.
Diabetes management requires maintaining hemoglobin A1c levels below 7% for most patients. Newer medications like SGLT2 inhibitors show promise in protecting kidney function while controlling blood sugar.
Dietary modifications play a crucial role in CKD management. Reducing sodium intake helps control blood pressure and fluid retention. Protein restriction may be recommended in advanced stages to reduce kidney workload, though this requires careful monitoring to prevent malnutrition.
Managing complications becomes increasingly important as CKD progresses. This includes treating anemia with iron supplements or erythropoiesis-stimulating agents, managing bone and mineral disorders with vitamin D supplements and phosphate binders, and addressing cardiovascular risk factors.
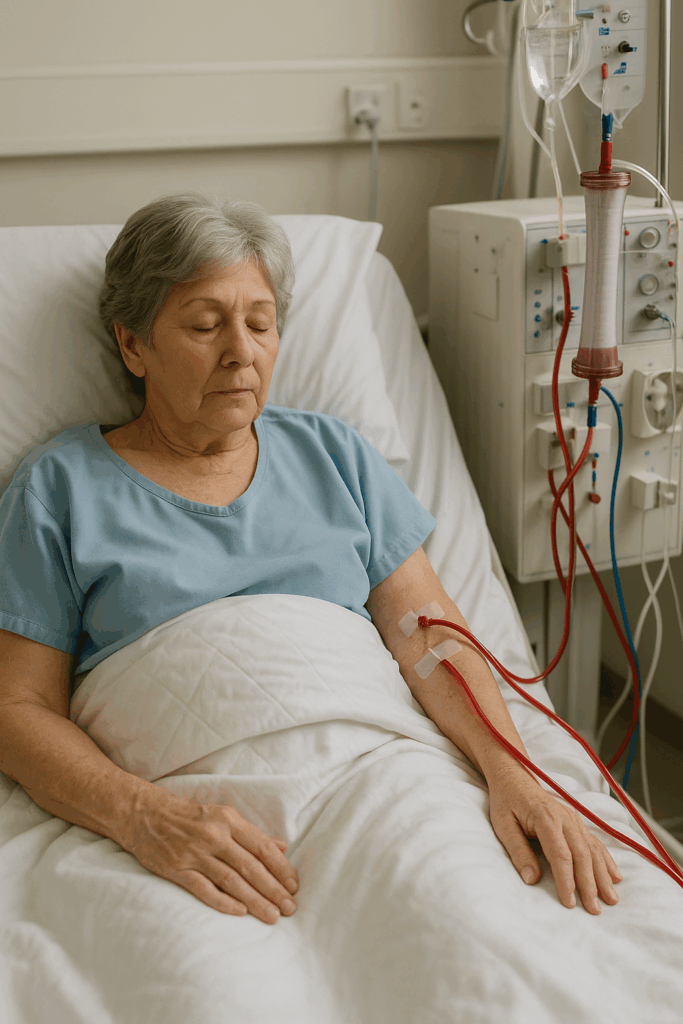
For end-stage kidney disease, renal replacement therapy through dialysis or kidney transplantation becomes necessary. Early planning for these treatments improves outcomes and quality of life.
Prevention Strategies: Protecting Your Kidneys
Prevention remains the most effective approach to CKD. Maintaining healthy blood pressure through regular exercise, weight management, sodium reduction, and medication compliance are the foundations of kidney protection.
Diabetes prevention and management through lifestyle modifications and appropriate medical care significantly reduces CKD risk. Regular monitoring of blood sugar, blood pressure, and kidney function allows for early intervention when problems arise.
Avoiding nephrotoxic substances, including excessive NSAID use, staying hydrated, and not smoking all contribute to kidney health. Regular medical check-ups enable early detection and treatment of conditions that could lead to CKD.
Understanding chronic kidney disease empowers older adults to take proactive steps in prevention and to look for appropriate care when needed. With proper management, early detection, and comprehensive care, many people with CKD can maintain a good quality of life and slow disease progression.








The U.S. Public Health Service: Guardians of America’s Health
By John Turley
On July 3, 2025
In Commentary, History, Medicine
The United States Public Health Service (USPHS) has quietly served as the backbone of the nation’s public health infrastructure for over two centuries. From its beginnings as a maritime medical service to its current role as a comprehensive public health organization, the USPHS has evolved to meet the changing medical challenges facing Americans and to protect and promote the health of the nation.
Origins and Early History
The U.S. Public Health Service traces back to 1798, when President John Adams signed “An Act for the Relief of Sick and Disabled Seamen.” This legislation established the Marine Hospital Service and created a network of hospitals to care for the merchant sailors who served America’s growing maritime commerce. The act represented one of the first examples of federally mandated health insurance, as ship owners were required to pay 20 cents per month per sailor to fund medical care.
The Marine Hospital Service initially operated a series of hospitals in major port cities including Boston, New York, Philadelphia, and Charleston. These facilities served not only sick and injured sailors but also played a crucial role in preventing the spread of infectious diseases that could arrive on ships from foreign ports. This dual function of treatment and prevention would become a defining characteristic of the USPHS mission.
The transformation from the Marine Hospital Service to the modern Public Health Service began in the late 19th century. In 1889, the organization was restructured and placed under the supervision of Dr. John Maynard Woodworth as Supervising Surgeon—later Surgeon General—marking the beginning of its evolution into a more comprehensive public health agency. The name was officially changed to the Public Health and Marine Hospital Service in 1902, and finally to the U.S. Public Health Service in 1912, reflecting its expanded mandate beyond maritime health.
Evolution and Expansion
The early 20th century brought significant expansion to the USPHS mission. The 1906 Pure Food and Drug Act gave the service regulatory responsibilities, leading to the creation of what would eventually become the Food and Drug Administration. During World War I, the USPHS took on additional responsibilities for military health and epidemic control, establishing its role as a rapid response organization for national health emergencies.
The Great Depression and World War II further expanded the service’s scope. The Social Security Act of 1935 created new public health programs administered by the USPHS, while wartime demands led to increased focus on occupational health, environmental health hazards, and the health needs of defense workers. The post-war period saw the establishment of the National Institutes of Health—originally called the Laboratory of Hygiene—as part of the USPHS, cementing its role in medical research.
Major Functions and Modern Roles
Today’s U.S. Public Health Service operates as part of the Department of Health and Human Services and supports major agencies and functions. The service’s mission centers on protecting, promoting, and advancing the health and safety of the American people through several key areas.
Disease Prevention and Health Promotion are the core of USPHS activities. It works with the Centers for Disease Control and Prevention (CDC), to lead national efforts in the prevention and control of infectious and chronic diseases. From tracking disease outbreaks to promoting vaccination programs, the USPHS a part of America’s first line of defense against health threats.
Regulatory and Safety Functions represent other crucial areas. The USPHS coordinates with the Food and Drug Administration (FDA) to ensure the safety and efficacy of medications, medical devices, and food products. It works with the Agency for Toxic Substances and Disease Registry monitoring environmental health hazards. Other USPHS components are involved in regulating everything from clinical laboratories to health insurance portability.
Emergency Response and Preparedness has become increasingly important in recent decades. The USPHS maintains rapid response capabilities for natural disasters, disease outbreaks, and public health emergencies. This includes the deployment of Commissioned Corps officers to disaster zones and the maintenance of strategic national stockpiles of medical supplies.
Health Services for Underserved Populations continues the service’s historic mission of providing care where it’s most needed. The Health Resources and Services Administration oversees community health centers, rural health programs, and initiatives to address health disparities among vulnerable populations. The Indian Health Service is an important part of the USPHS, providing healthcare to often isolated communities.
The Commissioned Corps
One of the most distinctive features of the USPHS is its Commissioned Corps, a uniformed service of over 6,000 public health professionals. Established in 1889, the Corps operates as one of the eight uniformed services of the United States, alongside the armed forces, NOAA Corps, and Coast Guard. Officers hold military-style ranks and wear uniforms, but their mission focuses entirely on public health rather than defense.
The Commissioned Corps provides a ready reserve of highly trained health professionals who can be rapidly deployed to address public health emergencies. From hurricane and disaster relief to pandemic assessment and treatment, Corps officers have served on the front lines of America’s health challenges, providing everything from direct patient care to epidemiological investigation and public health program management.
Contemporary Challenges and Future Directions
The U.S. Public Health Service continues to evolve in response to emerging health challenges. Climate change, antimicrobial resistance, mental health crises, and health equity concerns represent current priorities. The COVID-19 pandemic demonstrated both the critical importance of robust public health infrastructure and the challenges of maintaining public trust in health authorities.
As America faces an increasingly complex health landscape, the USPHS mission of protecting and promoting the nation’s health remains as relevant as ever. From its origins serving sailors in port cities to its current role addressing global health threats, the U.S. Public Health Service continues its quiet but essential work of safeguarding American health, adapting its methods while maintaining its core commitment to serving the public good.
The service’s history shows that effective public health requires not just scientific expertise, but also the institutional ability to respond rapidly to emerging threats, the authority to implement necessary interventions, and the public trust to lead national health initiatives. As new challenges appear, the USPHS continues to build on its more than two-century legacy of service to the American people.